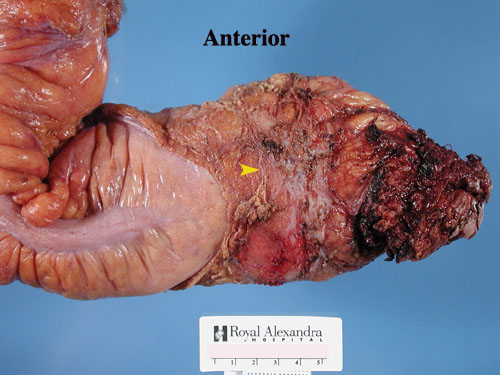
Here are 2 additional examples of TME. The first shows grade 3 mesorectal excision. Note the smooth surface. This is an AP resection thus exposed levators at the distal margin is acceptable. The mesorectum doesn't go this low. The yellow arrowheads point to fine wisps of fascia on the anterior and posterior surfaces. This ensures that the surgeon is in the correct plane. The third image is also a grade 3 and shows the natural midline posterior cleft that has been christened "the mesorectal buttocks". An example of grade 1 is also demonstrated.
Grade 3 mesorectal excision
Grade 3 mesorectal excision, anterior view
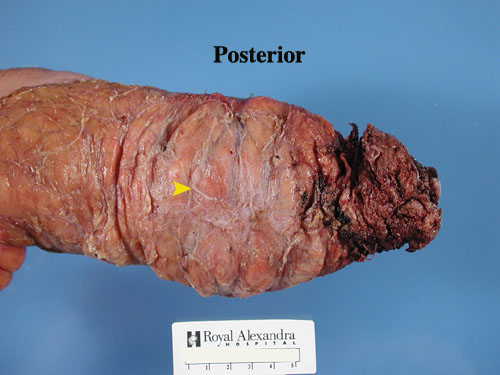
Grade 3 mesorectal excision, posterior view

Grade 3 mesorectal excision, posterior view demonstrating the mesorectal buttocks.
Grade 1 mesorectal excision
The case illustrated below shows a ragged distal end
with exposed muscularis propria (yellow arrowhead). Cut surfaces
clearly show the loss of surrounding mesorectum. It is no surprise
that the distal margins have a tendency to become ragged since the surgeon
has to essentially make a 90 degree turn from the plane that he is following
so that he can ensure complete mesorectal excision up to the distal line
of resection. This is apparently not easy. Considering that
there may be fat with tumour deposits left behind, comparison to some of
the other images on this website should make it fairly clear why patients
like this are at increased risk for recurrence.

Slices through the tumour site show the exposed muscularis propria (yellow arrowhead). The red arrow shows tumour extending close to the anterior resection margin. We see lymph node deposits in the upper left corner. This is proximal to the tumour. It is quite possible there may be tumour deposits at the 9 o'clock position that have been left behind in the more distal slices.

TME main page
Method of dissection of colorectal
adenocarcinoma
Additional examples of TME
Bach home