| . | |||
| MEDICINE IN CAPE TOWN | |||
| Physicians in South Africa might go into medicine with idealistic dreams of helping the sick, then train in the public sector where they do have to do a year of community service in a rural place and then enter residency programs where as "registrars" they have the idealism systematically ground out of them by years of struggling with inadequate resources against the overwhelming mass of desperately sick patients that never stop coming through the door. Sounds rough, doesn't it; no wonder many head for private practice or even flee the country for other western nations, where these English-speaking, highly trained and experienced physicians are prized as welcome guests for much higher pay. In fact, medical students from abroad often come to South Africa for the rigorous training and intense experience, particularly in emergency medicine and surgery. As a patient, if you are penniless you get the public system, and if you have any money at all you will buy into one of the literally hundreds of private health care insurers, ranging from extremely low-rent plans which provide effectively no coverage all the way to super deluxe plans for the extremely wealthy. Private health care doesn't necessarily provide better care, as pointed out by Roal -- for at a private hospital you might be one of twenty or thirty patients under the care of one experienced internist, but his attention turns many places and he might only physically be in house once a day, meanwhile at a public teaching hospital there are interns and house officers and students and staff onsite all the time. But the private system certainly offers a deluxe experience, much in the way that the "Postnet" courier service is more pleasant than the post office -- 3x the price but shorter lineups, faster service and a general lack of those pesky black people (a feeling that hopefully fewer and fewer people are allowing themselves these days). In Groote Schuur hospital, the public radiology department on "C" floor has a 1- and 4-slice CT scanner, crowds in the waiting room ands and some quite antique X-ray equipment, while upstairs in the private department (staffed by the same radiologists on different days), there are softly carpeted floors, flat-screen LCD monitors on the computers, and nicer viewboxes. Is the diagnosis any better on the private floor? Not necessarily…although sometimes, particularly in radiology, technology is critical. Radiologists on the private side do sometimes help out the public -- for example a private clinic graciously donated scan time on a 64-slice scanner for an important CT angiogram on a child with Takayasu aortitis, since none of the public-system CT scanners were fast enough to do the scan. | |||
 Old-school "digital" |
 Triage |
 Single-slice CT scanner at Red Cross Hospital |
|
| . | |||
| . | |||
CAPE TOWN HOSPITALS | |||
| Groote Schuur hospital (GSH) is one of the largest teaching hospitals in Cape Town, rebuilt to a capacity of ~2000 beds in the 1980's at about the same time as the University Hospital in Edmonton was built, with a similar layout including a mechanical floor between each "real" floor which means walking a lot of stairs. In the 1960's, GSH was the site of the first heart transplant in the world, and it is still a big transplant centre. But also in the 1960's, GSH had separate entrances and separate wards for black and white patients. The location is fantastic, backing onto Table Mountain with a panoramic view of Cape Town, close to wealthy suburbs and far from the townships. Parking is tightly controlled and if you can't get a pass for the parkade, it's not just inconvenient, it's unsafe -- you have to walk a few blocks outside the hospital at uncertain hours in not the best neighborhood, and incidents happen. I was told that one cause for these parking-lot muggings is that patients, once discharged, have no way to get back to their homes in the townships and get cash any way they can. Urban legend? Anyway, the hospital itself is spacious and comfortable, with lecture theatres and a snack shop, several eating areas and air conditioning. As a tertiary hospital, patients can't get here without referral from a secondary hospital, so the problems are highly filtered and patients very complex. | |||
 Groote Schuur Hospital -- new on the left, old building at right |
 White entrance and wards on the right, blacks on the left |
 View from GSH entrance |
|
 Spacious modern GSH main hallway |
 Could be 1st world -- but don't look at the public bathrooms here! |
 Maternity ward |
|
| . | |||
| Diana's hospital, New Somerset Hospital (NSH), is next to the Waterfront, a vast tourist development of expensive restaurants, tony shops and an Imax theatre at the harbor surrounded by $400+/night hotels. The original yellow building is not in much use, and in fact a recent sweep was done to kick out the many vagrants who had started living in its corners and attics. The newer concrete monolith that is the actual hospital serves a mix of poor white and black people, with a triage area resembling a large jail cell -- gates bar the way into the E.R., manned by security guards aiming to prevent gangs from finishing off the job on wounded assault victims. Nearly everyone at NSH has tuberculosis -- Diana's medicine team admitted ~12 patients per night and 10-11 of these would have TB, most also with HIV. Most people deny that they are HIV positive, or say they "don't know", because of the social stigma associated with it. The polite euphemism for the medical charts is "RVD+" (RetroViral Disease). So overwhelming is the burden of TB that there is essentially no isolation -- a patient with multi-drug-resistant TB (MDR-TB), who in Canada would be isolated in a room with negative pressure ventilation drawing air carefully through a safe path and examined by a team wearing special masks, gowns and gloves, in South Africa is probably in a common ward room with 6 other patients and the medical staff don't even bother with masks. But relax, almost everyone else in the room has TB already. A sample of the fluid building up beside the lungs is drawn from a large needle placed with virtually no precautions, just an alcohol swab on the skin. | |||
 "Old" New Somerset Hospital, with Table Mountain behind. |
 New building -- somewhat less attractive and soon to be bulldozed for the soccer stadium anyway. |
 Yes, there is an air ambulance -- but you probably have to be VIP to get this treatment |
|
 Hospital ward at NSH |
 Draining a pleural effusion -- with minimal sterile precautions! |
||
| . | |||
| NSH is an urban secondary hospital, whose sickest patients (those without garden-variety HIV and TB) would be sent to GSH. The largest secondary hospital in the townships is GF Jooste, which is totally overrun with patients. In a typical night on internal medicine in the main Edmonton tertiary hospital, a resident would admit 5-10 patients; at Jooste, it's 30 patients a night, many with a complex mix of HIV, TB, and side-effects from the multiple drugs being given for those diseases. Plus a wide selection of trauma. Luckily, Jooste is benefiting from government priorities, which are to "bring health care to the people" by putting resources into primary and secondary hospitals. This means Jooste, and rural hospitals like Vredenberg, 50 km from Cape Town, are getting new equipment and facilities, while the tertiary hospitals (which still serve mostly black people but which might mistakenly be thought to be serving whites since they are in white areas) are left with budget cuts despite strenuous opposition. | |||
 GF Jooste Hospital |
 Nice neighborhood |
 Rushing in E.R. |
|
 Vredenberg, 1 hour drive north of Cape Town |
 Beautiful new hospital |
 Spiffy new waiting room |
|
 Top quality equipment, not yet stolen |
 Sunny courtyard |
 Lovely little areas for patients to recuperate and relax |
|
 Salaries -- divide by 6 for Canadian dollars: nurse, $13,000; senior specialist physician, $57,000. |
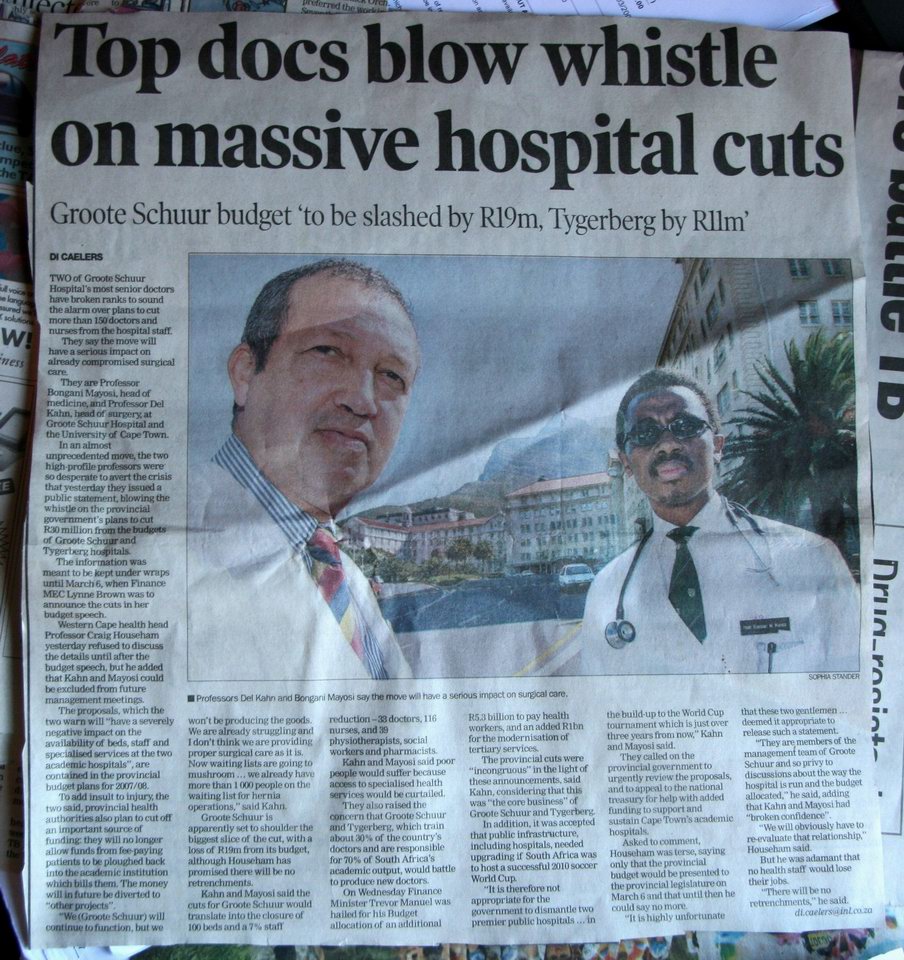 Going out on a limb to protest tertiary hospital cuts |
 Failure |
|
| . | |||
| The Red Cross Children's Hospital is the main tertiary hospital not only for Cape Town but arguably for nearly the entire continent of Africa. Any child sick south of Cairo would ultimately end up here if sick enough. It's a beautiful place, not far from GSH. Between devoted staff, wealthy donors and the general sense that one ought to help sick children, they have been able to sidestep the latest round of budget cuts and the financial situation overall seems a bit healthier than at GSH. The hospital really has a great work atmosphere and it's a pleasure to go there. | |||
 Cheerful Red Cross Hospital |
 And a fine location too |
 View across Rondebosch Common from Red Cross Hospital to Groote Schuur Hospital on the slopes of Table Mountain |
|
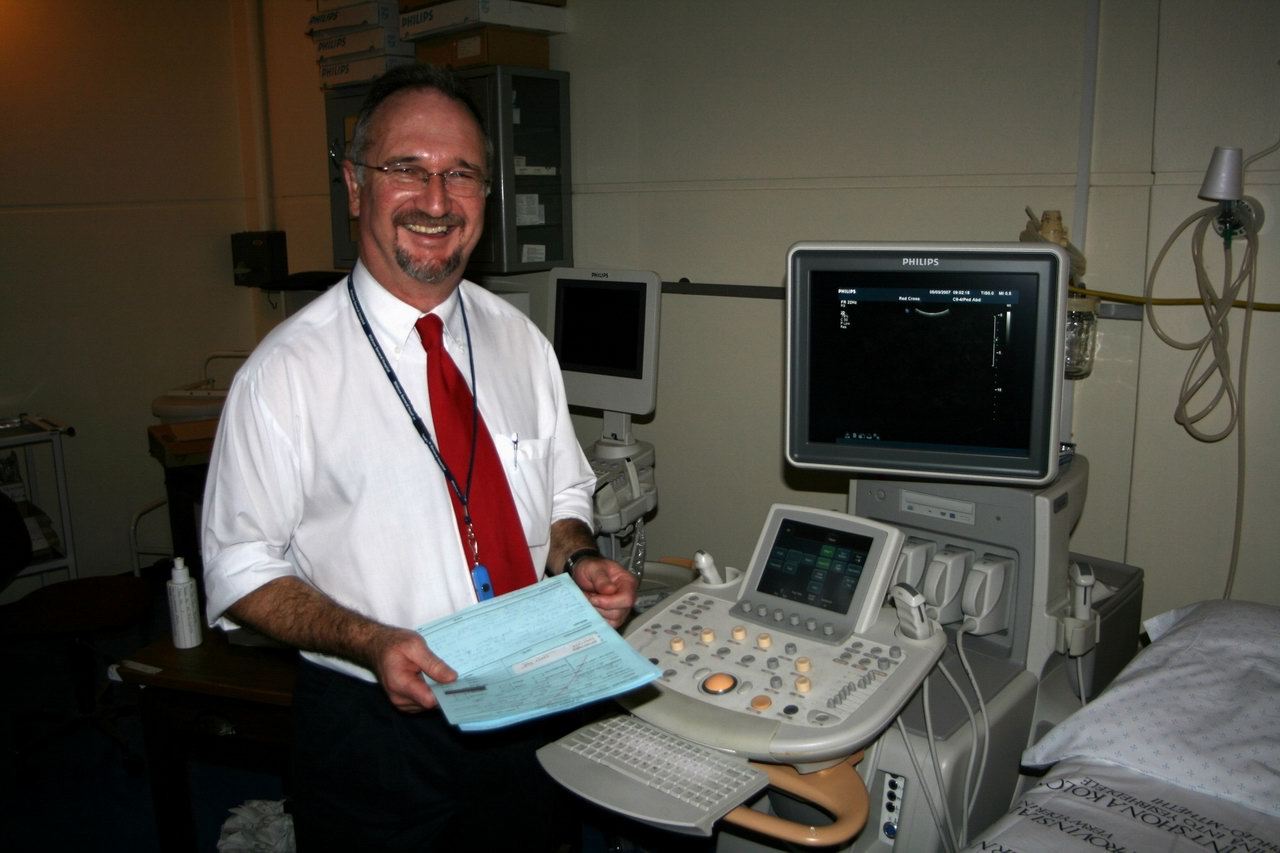 Dr. Dick Pitcher shows off the beautiful new Philips ultrasound machine, same as we have at home in Edmonton |
Single slice CT scanner is long past due for an upgrade |
 Great lunchroom! |
|
| . | |||
| The South African government is trying to force health care delivery by a model quite different than in Canada. In Canada we have been centralizing care -- instead of having multiple peripheral hospitals, we'd rather have a very good ambulance system bringing people to central tertiary-hospital beds, where the best specialists rapidly deliver critical care and the patient, his problems "sorted out", then is sent to a step-down hospital for continuing care during convalescence. Here, the opposite is happening: the ambulance system and tertiary hospitals are both being gutted, with funding increases for the smaller regional hospitals. The rationale, quite honorably, is that everyone deserves a minimum standard of medical care and many South Africans currently have no access at all. But, the South African way seems to be being done without consulting the doctors and nurses -- it's just not practical. No one really wants to work in an isolated setting without proper backup and resources, and it is virtually impossible to fill most staff positions with anyone other than the most junior and least skilled at any of these regional hospitals. An example: Jooste has the nicest CT scanner in the public system in Cape Town, with 6 slices, but it only has staff to run it from 8 AM to noon on weekdays. If this scanner had been installed at GSH, it would be running 24 hours a day for the complex problems it is designed for, with the radiologists to interpret the images and the surgeons to act on the pathology. At Jooste, the only radiologist seeing the scans is a resident like me, 4 hours a day, and the cases with anything interesting get referred on to GSH anyway, after some delay. So it is a strange way to allocate resources -- almost as bizarre as the donation of a portable MRI unit to Jooste. The MRI sits in a locked room because no one knows how to use it, and anyway even if they could figure it out, it can only be used to assess knees and other joints for which no surgeons have time to fix out there anyway. One doesn't know whether to laugh or cry... | |||
 CT techs at Jooste, probably smiling since their day is only 4 hours long |
 Brand new six slice scanner at Jooste |
 Portable MRI behind a locked door at Jooste, no good to anyone except as a tax deduction for the donor |
 Jooste sonographer shows how patients lie down for their ultrasounds |
| . | |||
| RADIOLOGY ROTATION | |||
| My one-month radiology rotation was an absolute pleasure, as the residents and staff welcomed me warmly right from the start. Doing an elective abroad as a senior resident, one year away from writing the final exams, is in my opinion a much better choice than traveling as a medical student. One knows a lot more and can actually contribute (I dictated numerous X-rays, especially in the pediatric hospital, and did a CT arthrogram of the shoulder since that afternoon I was the person in the department with the most experience). Seeing a different patient group and pathology at this stage is a great way to "shake up" one's medical knowledge -- for example I now have a much better sense of when to include TB in the differential diagnosis, and also of how important it is to think of TB or HIV. Even trauma is different in South Africa -- the people here have figured out that stabbing someone in the eye is very effective at crippling them, and while I have never seen this done in Edmonton I saw two in the same morning in Cape Town! | |||
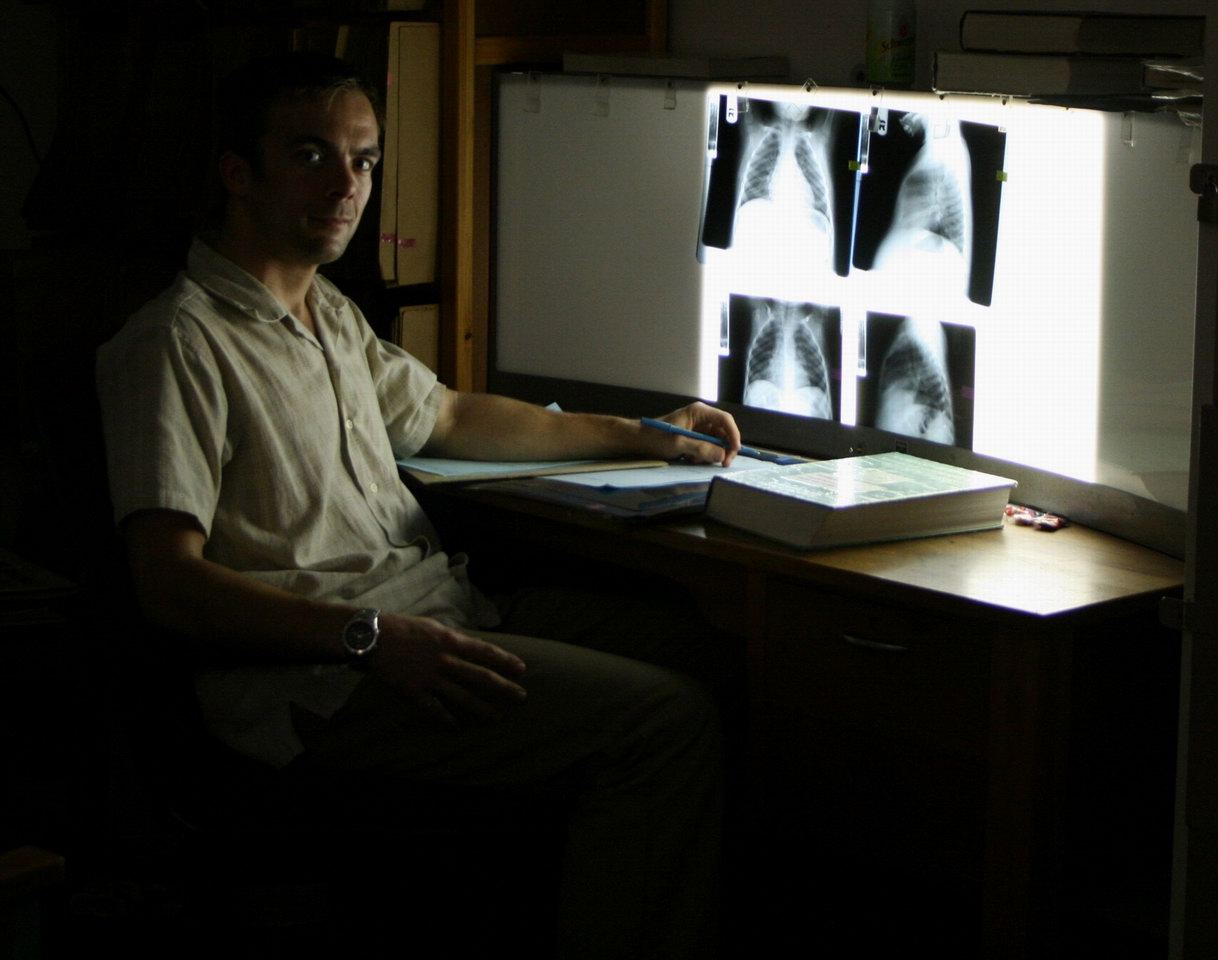 In the Red Cross reporting room |
 The standing girl was shy to get in the MRI; the boy lying in the machine is doing it to demonstrate to the girl how easy it is! She still refused to enter. |
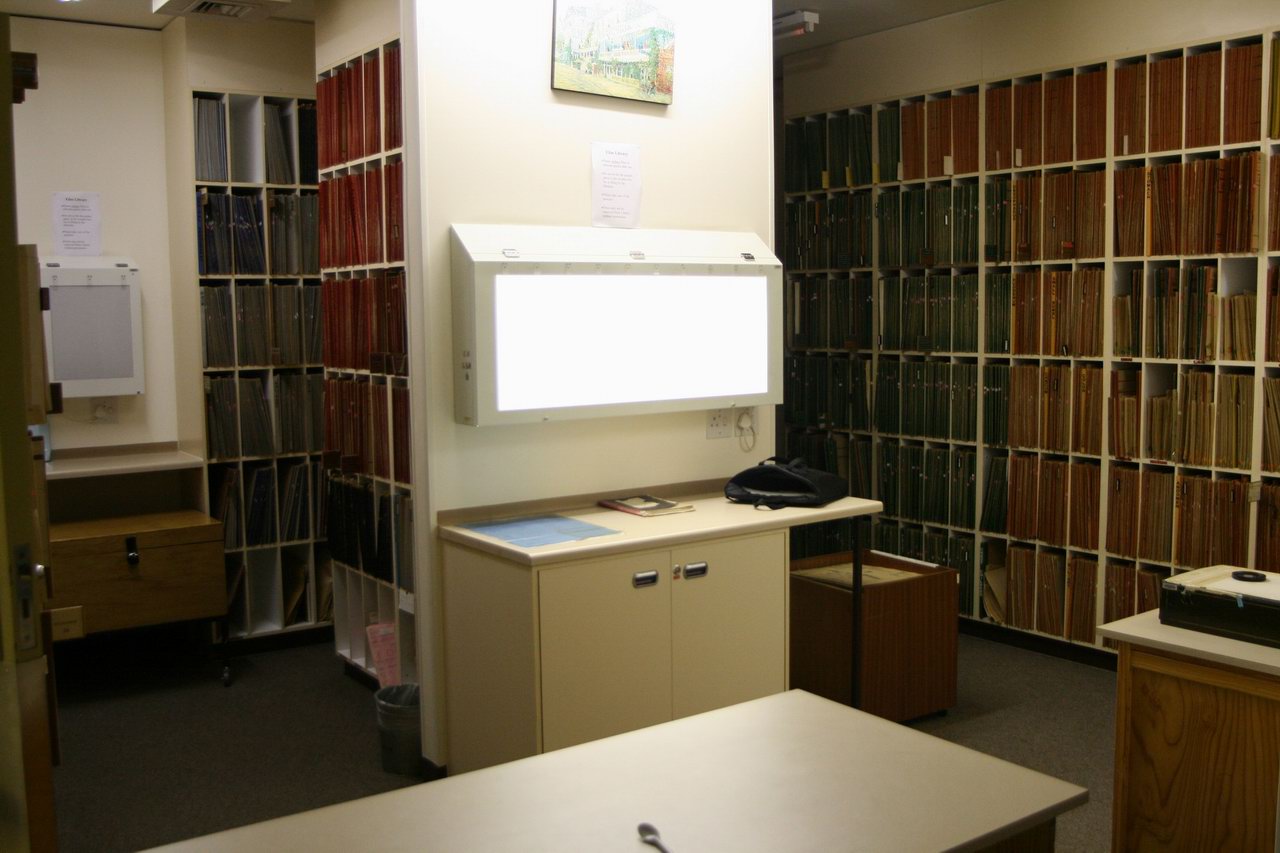 GSH film library -- fantastic reservoir of pathology. |
|
 Techs at GSH |
 Sandileh (2nd from R) joins the exodus of trained staff, but everyone keeps their spirits up |
 Registrars: Qonita, Ash, Dilesh and Himmel |
 Dilesh -- single and happy! |
| . | |||
| As Qonita and I observed, it is also a pleasure to see how much we think alike as residents/registrars, despite training on the opposite sides of the world. In a sense we shone mirrors on each other's programs, and could see the strengths and weaknesses of each. For example, the Edmonton program is strong in musculoskeletal and chest radiology and nuclear medicine, while GSH is particularly strong in hepatobiliary, vascular/interventional and neuro-imaging. The GSH group is currently struggling with the loss of several specialist consultants but coping remarkably well, and (for the moment) the training remains as good as what I have seen in Canada. The residents (registrars) at GSH have a great deal of clinical experience, as they have a more demanding call roster than we do and I think a higher volume of cases, particularly X-rays. They are good at taking responsibility, since they don't review all cases with their consultants but only the ones they find difficult or uncertain. This is intimidating at first -- if you miss something on an X-ray and are confident it is normal, no one else will ever look at it. Back in Canada, a staff radiologist also looks at the cases that are done, so it's more relaxing for the resident -- you feel that at least if you miss it, someone else will catch it. But I think a senior resident benefits from this (after all, if I pass my exams in a year I will be the only one looking at almost all the cases). It forces one to think about what abnormalities are likely to be important and those which are not. | |||
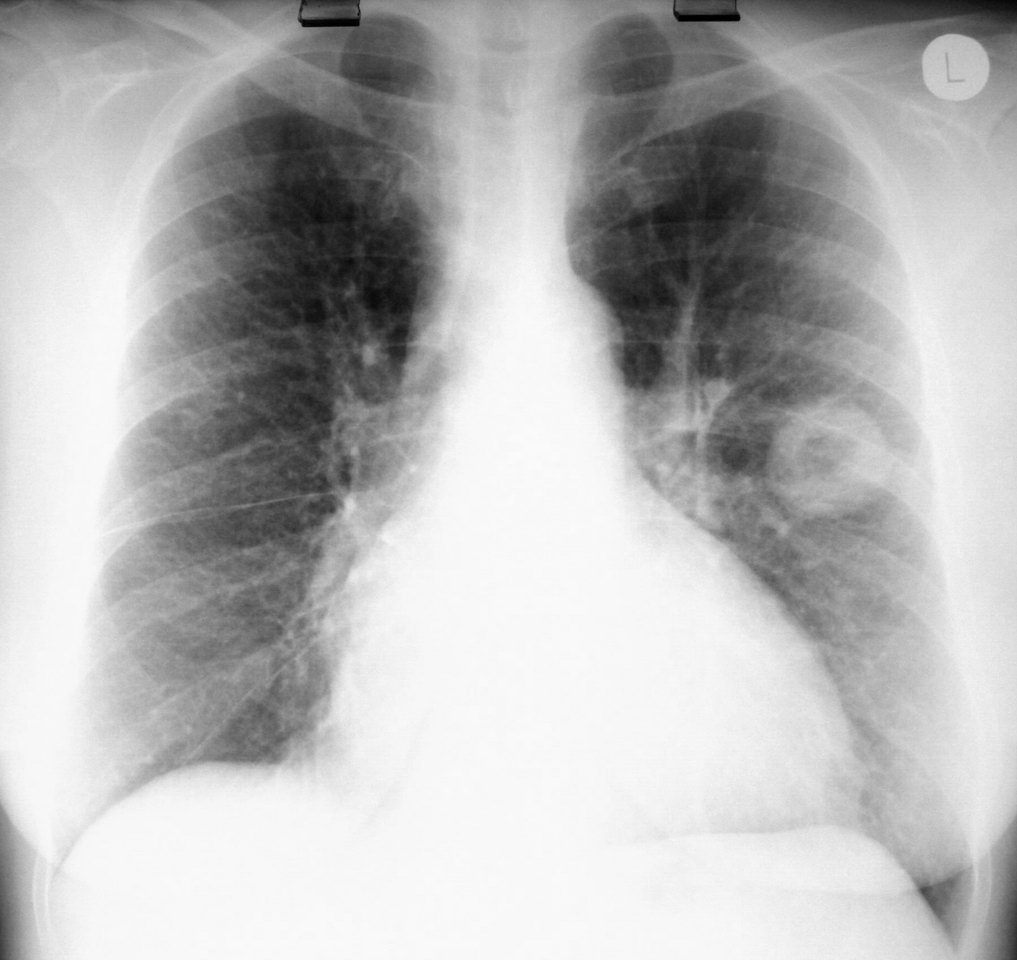
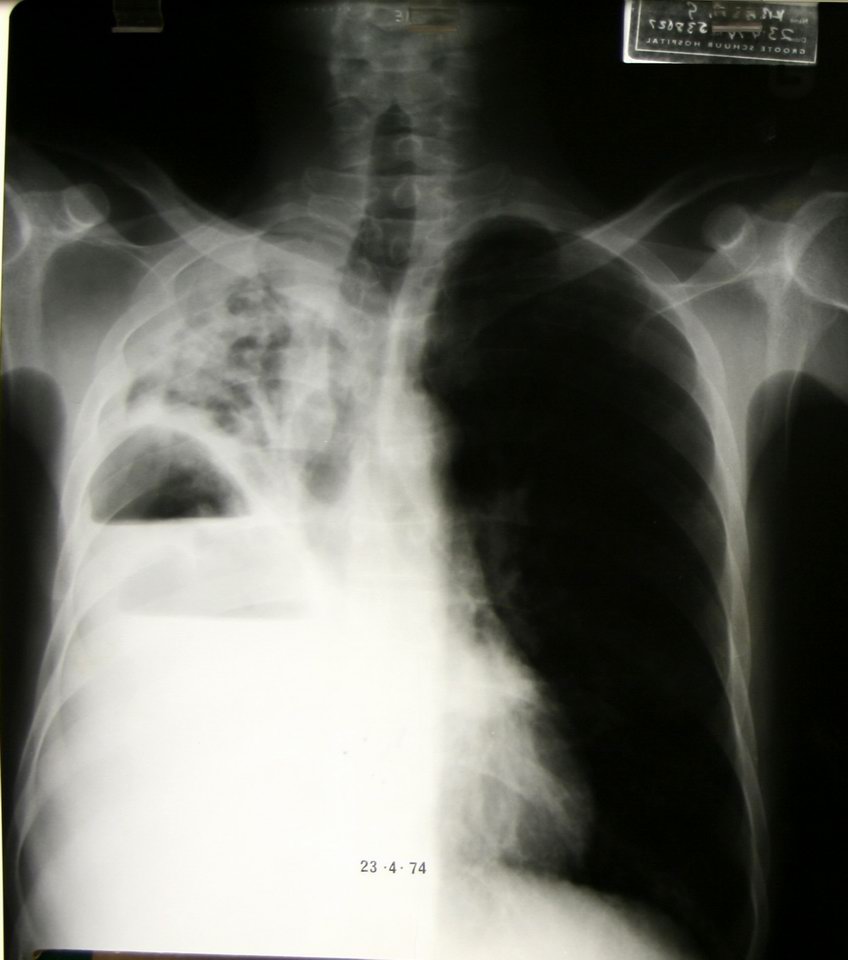 This patient has both a pulmonary abscess and an empyema at the same time! |
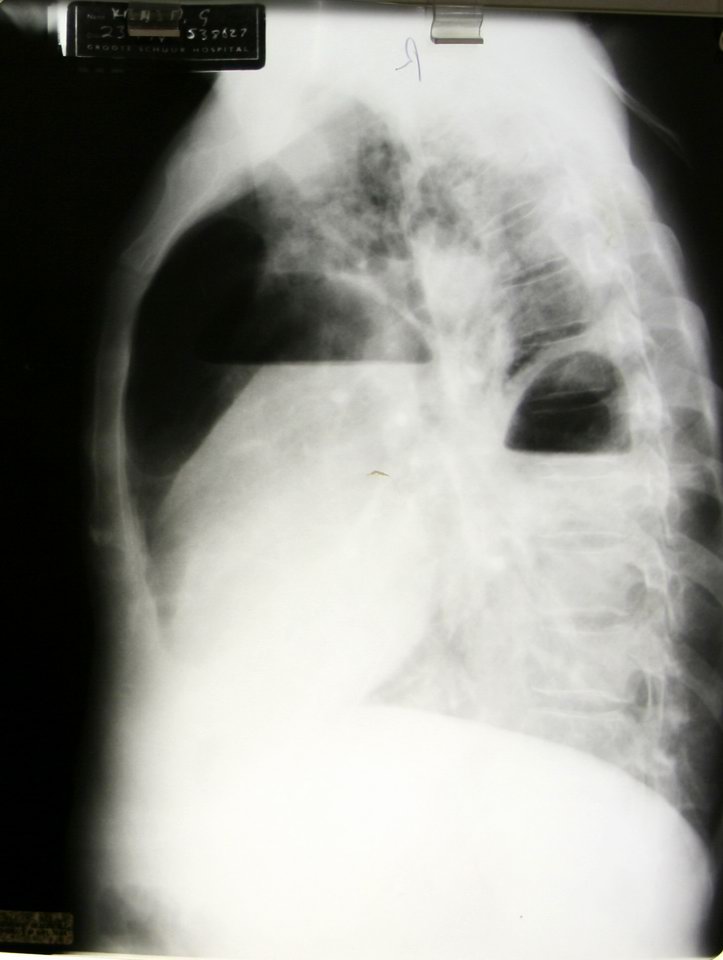 Lateral view, same patient |
 Madelung deformity -- a congenital problem with bone fusion in the arm |
 Patient with Madelung deformity -- worse on the left since she is left-handed. |
 Air in the skull from a stabbing -- "pneumocranium" |
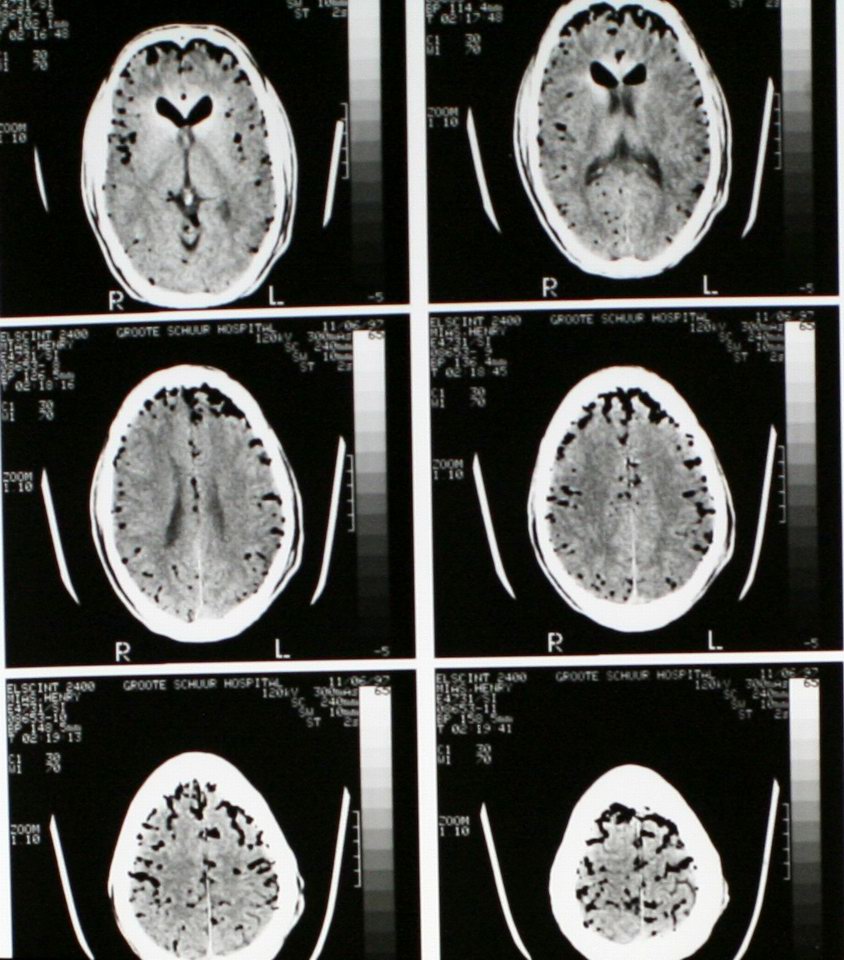 CT of same patient |
Prof Kottler, still going strong at mammo at age 80. |
|
| . | |||
| The GSH radiologists, like the South African radiologists I have met in Canada, have sharp clinical judgment. This is formed partly by the daily routine of a clinical meeting, where complex patients are discussed by the radiologists, surgeons and other specialists in a certain area -- e.g., hepatobiliary, pulmonary, vascular. I sat in on many of these meetings and watched some very good medicine happen, with radiologists often a close and valued part of the team making decisions. This role as respected and useful consultants is part of daily life and easily taken for granted until lost, as it often is in private or North American practice when the radiologist does the test and issues a report "in a vacuum". Without the constant feedback of the clinical meetings, the radiologist doesn't know what the referring physician wants to hear about in the report, and eventually that person loses respect for the radiologist, doesn't read the reports anymore, and maybe even tries to interpret their own imaging -- and then what is the point of being a radiologist at all? The meetings weren't always the idyllic mutually respectful sessions I am describing, with one in particular degenerating into a "test-the-radiologist" session. For this, the surgeons put up a series of films with little clinical history, which the entire surgical department had been discussing amongst themselves for days, and asked the radiologist to render a snap judgement -- then criticized the results and confirmed their stereotype that the radiologist is useless. The best clinical meeting I saw was the pediatric pulmonary meeting run by Dr. Pitcher, where everyone learned something from each other, patient care was the priority, and respect for everyone was in the air. That kind of working environment is worth a lot... |  Clinical meeting |
||
| . | |||
| Unfortunately, other aspects of being a radiologist in the public system in Cape Town are not so rewarding -- chief among these being budget restrictions and the previously mentioned bizarre purchasing priorities which result in a woeful lack of proper CT scanners in particular. The MRI unit is almost the same one as we have at home, a modern 1.5 T Siemens unit, but there is only one. And while the pediatric ultrasound department is justifiably proud of an ultra-modern machine as good as any back home, the ultrasound used in mammography looks like it was built in World War II. Again, this sharpens your skills as a clinician and radiologist -- when it's hard to get a scan done, you really think about whether it needs to be done, and when the equipment is old and slow you have to be more careful about your technique. The registrars are also more adept at hands-on things, since they have to do all their own ultrasound scanning and start all their own IV's for CT scan contrast dye injections. The hands-on work can be hazardous -- two radiologists have caught TB recently, one case perhaps related to long and close contact in small rooms doing ultrasound procedures. The other case is almost certainly from doing "CT FNAB's" (Fine Needle Aspiration Biopsies). In these procedures, a long thin needle is placed under CT guidance into a mass within the lung, to extract a few cells for assessment under the microscope. If the mass is not a tumor it is usually a TB granuloma, and when this is punctured you can imagine the thousands of bacteria spraying into the air. No surprise, then, that the person doing a dozen CT FNAB's in a day, every week, would catch TB. | |||
 Antique mammo ultrasound, as tall as I am and probably as heavy as a small car |
 Modern 1.5 T Siemens MRI |
 Cavitating mass in L lung -- for fun, let's poke this with a needle and see if we catch TB! |
|
| . | |||
| INTERNAL MEDICINE ROTATION | |||
| Diana's experience in internal medicine was dominated by HIV and TB, in a very busy clinical environment. Dr. van zyl Smit (Roal) organized visits to Jooste and Vredenberg hospitals (the latter was a fine day trip which I also went on and which culminated in a delicious dockside lunch in Saldanha!) and some wondrous pathology was on offer. If you are proud and penniless and haven't got a car, it's amazing how sick you will let yourself get before finally seeking help -- often much too late for anyone to do anything. Fortunately, the government has recognized that antiretroviral drugs do prevent HIV, reversing an earlier stance that could be summarized as "let them die" -- and even life insurance companies have just agreed not to deny claims based on HIV status, as long as people show that they have sought treatment. Patients are very, very sick and the cases are often very sad; Diana often had weighty tales to tell at night and I was thankful again for my choice of radiology as a field. Roal and the incredibly talented Dr. Ntusi, a resident who should have been a Rhodes scholar in Diana's opinion, held the fort together and it was an intense and mind-broadening experience for Diana. | |||
 Dr. Ntusi gives a talk. That's Dr. Sally Candy, neuroradiologist, watching in front. |
 Dr. Ntusi, star resident, and Dr. Mayosi, head of GSH internal medicine (see the front page of the newspaper article above) |
 Diana's team |
|
 Valerie takes blood for HIV testing |
 NSH medical team |
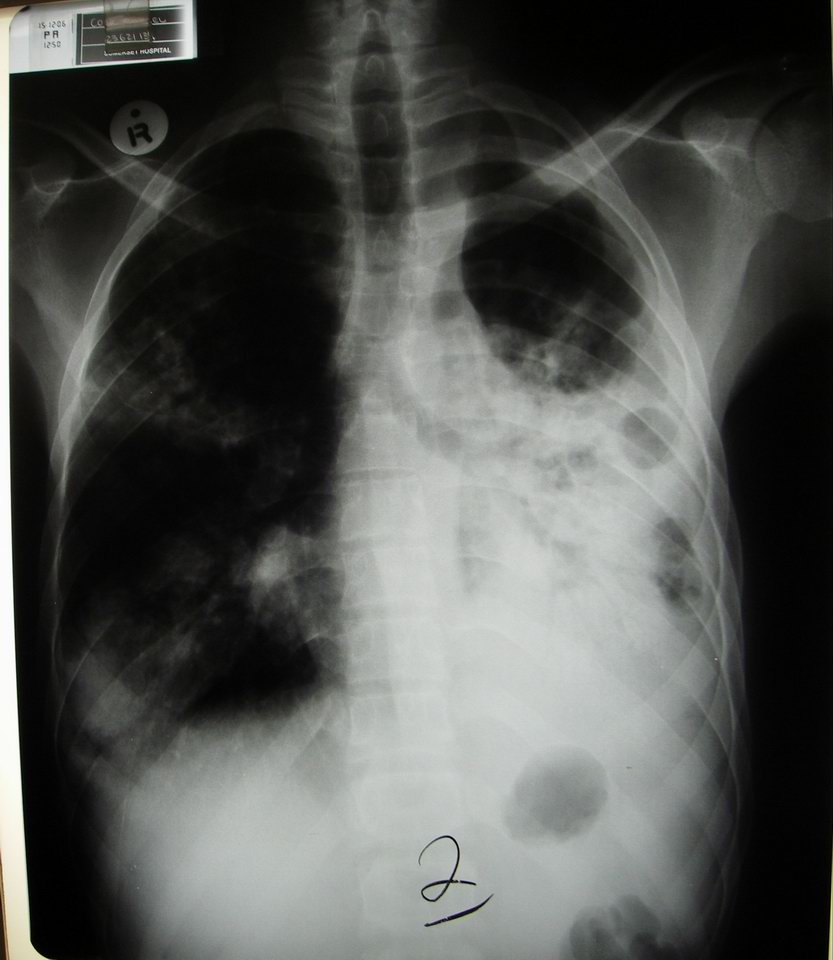 TB destroys another lung |
 Examining multi-drug-resistant TB patient. Note the total lack of isolation precautions. |
. |  Relaxing lunch in Saldanha |
 Diana gives her opinion of escargot! |
| . | |||
PREVIOUS |
NEXT |
HOME |
|