1. What are cognitive behavioural therapies? Why is understanding cognitive processes important?
2. Describe the three waves of cognitive behavioural therapy.
3. What are the assumptions and focus for cognitive restructuring therapies?
4. What is REBT? Describe the A-B-C-D-E paradigm, and explain how REBT is used to modify irrational beliefs?
5. What is Cognitive Therapy? What are automatic thoughts and some common cognitive distortions? How does Cognitive Therapy use hypothesis testing to evaluate a client’s beliefs?
6. What are the assumptions and focus for cognitive coping skills training?
7. What is Self-Instructional Training? Describe the basic steps in training.
8. What is Stress Inoculation Training? Describe the phases of training.
9. What are the pros and cons of cCBT?
10. How effective is each therapy?
11. What are the future challenges for behaviour modification? What can you do with this b-mod stuff?
Cognitive behavioural therapies (CBTs) combine cognitive and behavioural techniques to help clients to:
• understand problems
• see patterns of __________ thought
• evaluate behaviours based on more ________ thinking
• teach new skills to promote self-regulation
Cognitive processes include:
• ________
• perceptions
• beliefs
• expectations
• attributions
• self-statements
Cognitive processes are important in many problem behaviours:
• clinical depression involves __________ related to hopelessness, pessimism, and low self-esteem
• people become fearful of highly publicized but unlikely events
• people _______ about pain tend to rate their pain as higher
• highly aggressive people make hostile attributions about the intent of others
• explicit ______ systems allow us to be aware of those situations we fear and consciously think about them
• Skinner (1953):
- gave behavioural interpretations of psychoanalytic terms, like repression
- wrote about “________ behaviour analysis” which was about applying radical behaviourism to outpatient adult behaviour therapy (not hospital populations)
• in the 1950s, dissatisfaction with the vagueness of Freudian psychoanalysis and the paucity of ________ of its effectiveness was growing
• the term “_________ _______” emerged in the late 1950s:
- included using operant conditioning to modify overt behaviours
- and applying respondent conditioning to treat anxiety disorders
• Association for Advancement of Behavior Therapy (AABT):
- formed in 1966
- began publishing Behavior Therapy in 1970
- changed name to Association for Behavioral and Cognitive Therapies (ABCT) in 2005
• the cognitive revolution in the 1960s increased emphasis on cognitive processes
• by the 1970s, therapists focused on treating dysfunctional behaviours by changing the thought patterns believed to underlie them
• these approaches came to be known as “cognitive behaviour modification” or “_________ _________ therapies”
• examples include REBT and CT (see below)
• emerged in the early 2000s, emphasizing mindfulness, acceptance, values, goals, and thinking about your thoughts
• examples include Acceptance and Commitment Therapy (ACT) and Mindfulness-Based Cognitive Therapy (MBCT)
Assumptions:
• people interpret and react to events in terms of their perceived significance
• _________ deficiencies can cause emotional disorders
Focus of therapy:
• changing faulty ________ patterns/reducing dysfunctional thought processes directly
• or indirectly through overt behavioural interventions
e.g., arguing for a political position you do not favour makes you more favourably disposed to it
(Albert Ellis, b.1913-d.2007, the second most influential psychotherapist in history)
- developed to help individuals change __________ thoughts (Ellis, 1962)
- based on the assumption irrational interpretations predict that certain events will be emotionally unpleasant
- A-B-C-D-E paradigm (Ellis & Dryden, 2007):
• Activating events occur
• _______: our (irrational) interpretations about what the activating events mean
• Consequences: cognitive, behavioural, and emotional reactions to the activating events, interpreted through our beliefs
• _______ (refute, challenge, and question) irrational beliefs in therapy
▸ empirical/scientific dispute: Ask yourself “Where is the evidence that this belief is true?”
▸ __________ dispute: Ask yourself “Is my irrational belief helping me or does it make things worse for me?”
▸ logical dispute: Ask yourself “Is this belief logical? Does it ring true to common sense?”
• _________ relief follows recognition of the irrationality of one’s beliefs
- three main irrational beliefs (Ellis, 1994)
1. I must do well and win the ________ of others for my performances or else I am no good.
2. Other people must treat me considerately, fairly and kindly, and in exactly the way I want them to treat me. If they don’t, they are no good and they deserve to be condemned and punished.
3. I must get what I want, when I want it; and I must not get what I don’t want. It’s ________ if I don’t get what I want, and I can’t stand it.
- procedures to modify irrational beliefs:
1. identifying thoughts based on irrational beliefs
2. ___________ the irrational beliefs
3. teaching client to replace thoughts based on irrational beliefs with thoughts based on rational beliefs
- therapist is _______________, working directively to challenge irrational thinking
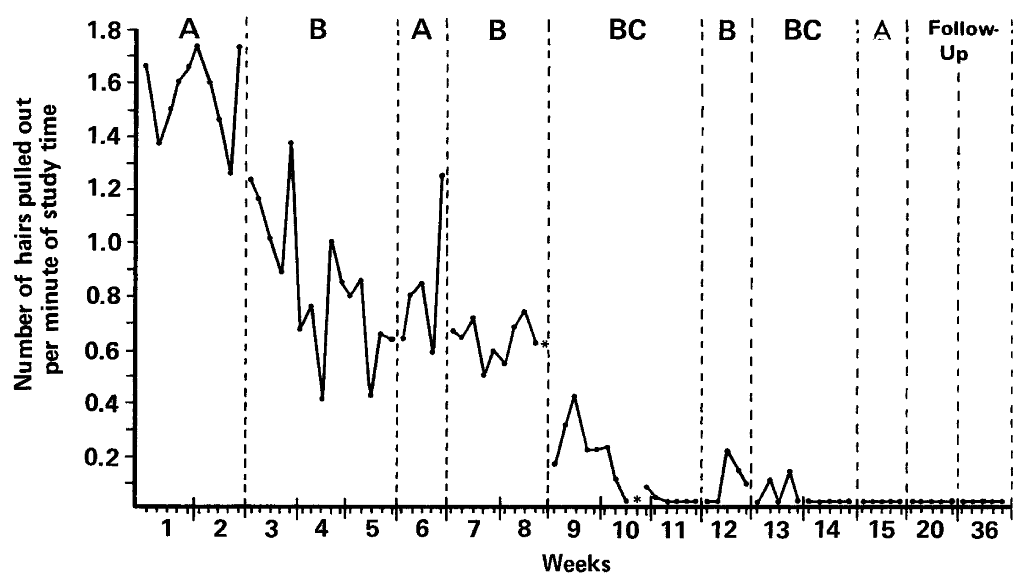
e.g., Bernard et al. (1983):
- 17-year old girl attending a private school
- asked for help with her ____-_______
• behaviour had been ongoing since age 12; she had to wear a wig to cover bald spots
• behaviour occurred when she was at home, studying schoolwork alone
• she felt worried, anxious, and depressed
- assessment revealed she made ____-_________ self-statements about school competence and approval from her father (e.g., “I can’t do homework.” “I am a failure.” “My father would be sad and that would be awful.”)
- REBT was used on her irrational cognitions
- results: target behaviour decreased to zero
(in BC phase, REBT was used with self-instructional training)
- effectiveness:
![]() has ______ empirical support
has ______ empirical support
e.g., REBT for alcohol abuse can change irrational thoughts, but there are limited changes in drinking
![]() is superior to no-treatment groups in treating anxiety
is superior to no-treatment groups in treating anxiety
![]() but is only equal to or less effective than other therapies (like exposure therapies or relaxation techniques)
but is only equal to or less effective than other therapies (like exposure therapies or relaxation techniques)
![]() many studies are ______ designed; REBT is often not operationally defined
many studies are ______ designed; REBT is often not operationally defined
![]() confrontational nature of REBT does not work well with clients who have certain disorders, like panic disorder or OCD
confrontational nature of REBT does not work well with clients who have certain disorders, like panic disorder or OCD
(Aaron “Tim” Beck, b.1921-d.2021, one of the ten most influential psychotherapists of all time)
- holds that faulty and negativistic _______ patterns lead to behavioural and emotional problems (Beck, 1972, 1976, 2020)
- beliefs are held in schemas that evaluate situations
- negative _________ thoughts: maladaptive (irrational) cognitions are automatically generated by distorted stored beliefs
- some common cognitive distortions (erroneous thought patterns; Burns, 1980):
• all-or-nothing thinking: viewing your personal qualities in extreme, black-or-white categories; if you’re not perfect, you’re a failure
e.g., a straight-A student who receives a B on an exam concludes that they’re a loser
• _______________: erroneously attributing an external event to yourself
e.g., you hear a group of people laughing, and you believe they are laughing at you
• jumping to conclusions: interpreting things as bad when there are no facts to support your conclusion
▸ mind reading: arbitrarily concluding that someone is reacting unfavourably to you
e.g., a friend (who was late) did not stop to talk to you, so you conclude that they must dislike you now
▸ fortune-telling: predicting that things will turn out badly
e.g., before a job interview, you tell yourself that you’re going to blow it
• __________________: drawing an overly general conclusion based on a single incident
e.g., after one failed attempt at painting a landscape, you believe that you will never succeed at painting landscapes or portraits, painting, art, or anything else
• magnification: exaggerating the meaning or impact of an adverse event
e.g., after receiving a paper with corrections on it, you believe that you are a terrible writer
• minimization: downplaying the meaning or impact of a beneficial event
e.g., scoring the winning goal, but thinking it was just luck
⚠ Note: Cognitive distortions may overlap, so that distorted thoughts may consist of more than one type of cognitive distortion.
- therapy applies collaborative __________: collaborative approach between client and therapist, using a hypothesis-testing approach to evaluate beliefs
• What is the ________ that supports a belief?
• What are some alternative explanations for a given distortion of cognition?
• What are the implications of an erroneous belief?
- client typically is assigned homework:
• evaluation of thoughts
• collection of ________ to test beliefs
• behavioural interventions, like relaxation exercises and activity schedules (written plan of daily activities that provides a sense of direction and control)
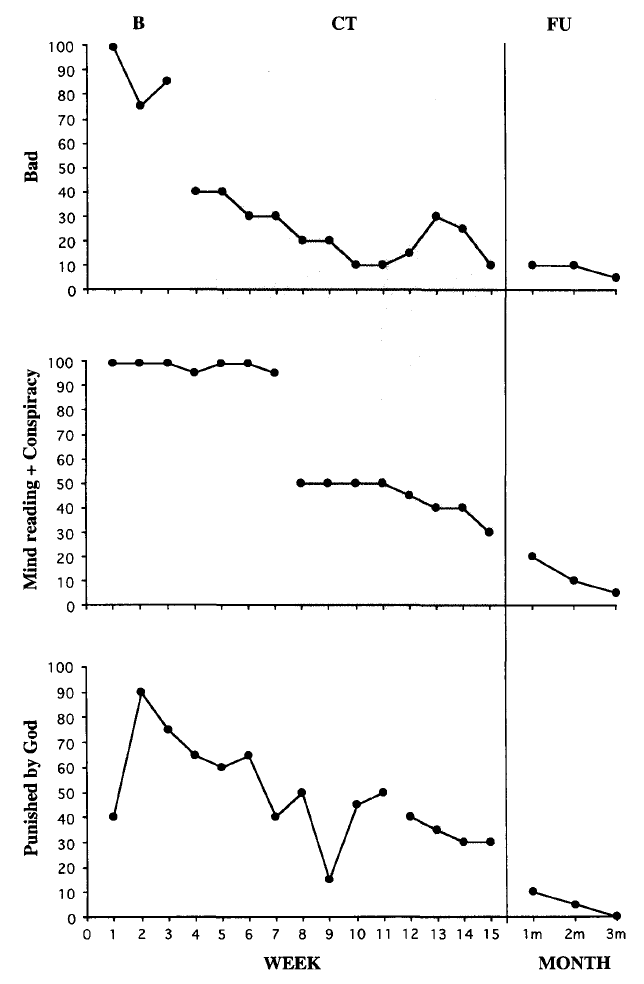
e.g., Chadwick and Trower (1996):
- 31-year-old man, living alone; diagnosed with schizophrenia
- experienced bizarre _________ (e.g., persecution and mind reading) and auditory hallucinations (hearing voices)
- believed that others could read his thoughts, God was punishing him for blasphemy
- had a depressive self-evaluative belief that he was a totally bad person
- CT was used on his beliefs
- results: conviction in his beliefs declined; was assessed as no longer having __________
- effectiveness:
![]() effective and durable in treating depression (at least as effective as __________)
effective and durable in treating depression (at least as effective as __________)
![]() may be least likely to work with those who have more severe depression
may be least likely to work with those who have more severe depression
![]() research on effectiveness with problems other than depression (anxiety disorders, personality disorders, delusions, substance use disorders) suggests the treatment is promising
research on effectiveness with problems other than depression (anxiety disorders, personality disorders, delusions, substance use disorders) suggests the treatment is promising
Assumptions:
• some problems are maintained by a deficit of adaptive cognitions
Focus of therapy:
• training new ________ skills
(Donald Meichenbaum, b.1940, voted one of the ten most influential therapists of the 20th century)
- initially developed to treat _________ children’s behaviours (Meichenbaum & Goodman, 1971)
- basic steps:
1. identify the problem situation, define desirable target behaviour to be increased, and identify competing behaviours
2. identify ____-____________ to be used in the problem situation;
- may include cue cards to use as prompts
3. use behavioural skills training to teach self-instructions
i) instructions: child is given deliberate strategy to follow
ii) ________: adult model performs task while using self-instructions
iii) _________: child practices task while verbalizing instructions aloud; instructions are gradually faded (whispered, then become covert)
iv) feedback: performance is immediately evaluated; praise or other reinforcers given for correct performance
e.g., Kendall and Braswell (1985)
- Peter, a 5-year-old in preschool for children with conduct and learning problems
- often did not complete his assignments; spent time looking around the classroom and daydreaming
- baseline performance:
• time spent paying attention to work: 31%
• problems correctly completed: 32%
- therapist taught Peter to use four specific self-instructions:
“What do I have to do first?” (problem __________)
“Circle all the words that begin with [a two-letter sequence].” (attention focusing and response guidance)
“Did I find all the words on the line?” (____-__________ and error correction)
“Good job. I found all of them.” (self-reinforcement)
- Peter’s performance measured by videotaping, and with a microphone used to record auditory self-instructions
- results:
• time spent paying attention to work: ___
• problems correctly completed: ___
- effectiveness:
![]() has been successfully applied to impulsive behaviours, schizophrenic behaviours, anger, _______, bulimia, and poor body image, as well as deficits in assertive behaviours, math problem solving, and cognitive and motor performance due to brain injuries (Spiegler & Guevremont, 2010)
has been successfully applied to impulsive behaviours, schizophrenic behaviours, anger, _______, bulimia, and poor body image, as well as deficits in assertive behaviours, math problem solving, and cognitive and motor performance due to brain injuries (Spiegler & Guevremont, 2010)
![]() less successful with social anxiety and personality disorders
less successful with social anxiety and personality disorders
![]() although primarily used with children, can also be used with adolescents and adults, and those with intellectual disabilities
although primarily used with children, can also be used with adolescents and adults, and those with intellectual disabilities
(Donald Meichenbaum, 1985, 1986)
- teaches cognitive skills that allow clients to deal with _________ events
- phases of training:
1. _________________ phase:
▸ therapist collaborates with client
▸ focuses on the nature of stress and how people respond to it
2. skills acquisition and rehearsal phase:
▸ teaches specific behavioural and cognitive coping skills such as progressive muscle relaxation (to alleviate stress-related muscle tension), desensitization, and coping statements
3. ___________ and follow through phase:
▸ involves practicing skills, and transition to real-world application of the skills
▸ can include modeling, role playing, and in vivo exposure to “inoculate” the client
e.g., Kaminer and Shahar (1987):
- Donna, a 32-year-old mother of two children
- was hospitalized for ____-__________, deeply scratching the left side of her face, which had been ongoing for 15 years
- stress inoculation training:
• phase 1/baseline: patient ____-__________ including a log of antecedents and recording target behaviour
• log revealed behavioural triggers: looking at a mirror, thinking about her scarred face, and anxiety-provoking thoughts of her abusive husband
• phase 2: patient was trained to use coping skills including progressive muscle relaxation, self-instructions, and self-administered ________ consequences (slapping the hand she used to scratch herself)
• phase 3: in week 4, patient visited her parents’ house to see her children and husband, whose behaviour caused a relapse in scratching
• patient practiced imaginary encounters with her husband, and was able to cope with a visit successfully, which marked a turning point
- results:
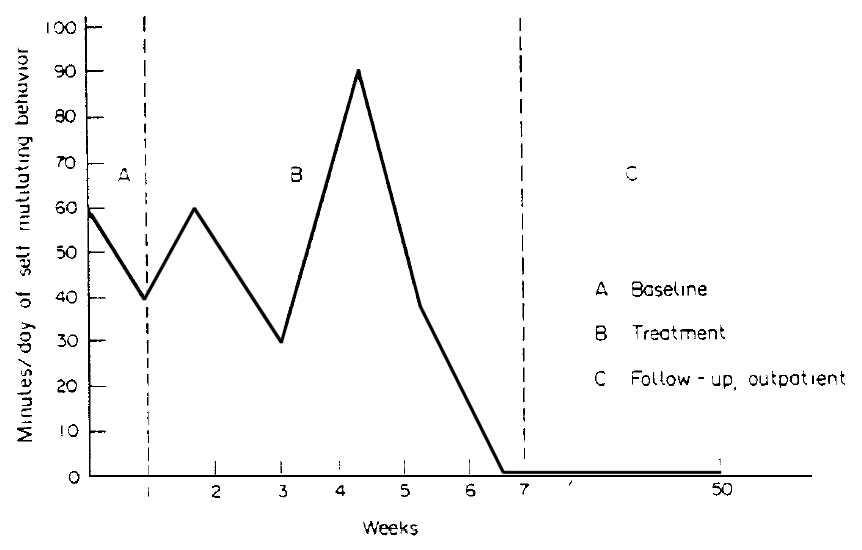
• at follow-up, Donna’s scar had healed, she held a full-time job for 6 months, and had ________ her husband
- effectiveness:
![]() many of the components (e.g., relaxation, modeling, desensitization) have been validated when applied independently
many of the components (e.g., relaxation, modeling, desensitization) have been validated when applied independently
![]() evidence suggests that this method is as effective as its _________ procedures
evidence suggests that this method is as effective as its _________ procedures
With increasing demand for psychotherapy, ________ include the limited number of therapists, and prohibitive costs of treatment.
One solution is computerized cognitive behavioural therapy (cCBT).
- the advent of AI chatbots has led to new opportunities for the application of cCBT (e.g., Woebot, Wysa, Youper)
- effectiveness:
![]() meta-analyses have shown that early versions of cCBT programs (e.g., MoodGYM®, Deprexis®) are somewhat effective for depression (Twomey et al., 2017)
meta-analyses have shown that early versions of cCBT programs (e.g., MoodGYM®, Deprexis®) are somewhat effective for depression (Twomey et al., 2017)
![]() narrative and systematic reviews of AI chatbot-based cCBT have shown substantial improvements in anxiety and depression (Farzan et al., 2025; Thakkar et al., 2024)
narrative and systematic reviews of AI chatbot-based cCBT have shown substantial improvements in anxiety and depression (Farzan et al., 2025; Thakkar et al., 2024)
![]() accessibility: cCBT is available 24/7; relatively low cost
accessibility: cCBT is available 24/7; relatively low cost
![]() ___________: can interact with millions of clients simultaneously
___________: can interact with millions of clients simultaneously
![]() interventions can be tailored to each individual
interventions can be tailored to each individual
![]() lack of therapeutic alliance: clients may have difficulty forming an emotional connection with a chatbot
lack of therapeutic alliance: clients may have difficulty forming an emotional connection with a chatbot
![]() _______ concerns (e.g., data privacy, algorithmic bias)
_______ concerns (e.g., data privacy, algorithmic bias)
![]() no data yet on long-term efficacy
no data yet on long-term efficacy
(Sarafino, 2012)
Challenges for behaviour modification
• enhancing the image of the field
- early conceptions of b-mod viewed it as ____, impersonal, and simplistic
- more recent attempts to change the image seem to have been successful
- recent work finds students rate teaching methods labeled as “behaviour modification” and “__________” equally acceptable
• closing the gap between research and practice
- a review of meta-analyses found “the evidence-base of CBT is very strong” (Hofmann et al., 2012, p.427)
- but empirically supported psychological treatments for psychiatric disorders are not being delivered to patients in routine clinical care
- a meta-analysis found that CBT was applied in a minority of cases (Shafran et al., 2009)
e.g., only 6.9% of patients with bulimia nervosa receive CBT
• integrating therapy approaches
- future work needs to consider combining __________ with behavioural approaches
- increasing promise shown in the area of prevention (e.g., smoking, drug use)
• future improvements
- more (and better) ________ supporting the effectiveness of b-mod, including randomized controlled trials
- more data on the cost-benefit ratios of b-mod, CBT, and cCBT
- addressing systemic racism, racial inequalities, and unique Indigenous issues (Levy et al., 2022; Melroe & Robbins, 2021)
Careers in behaviour modification
• assisting individuals with developmental disabilities as a Behaviour Interventionist
• teaching special _________
• clinical psychotherapy with cognitive and behavioural techniques
• work in industrial and organizational settings
• improving ______ behaviours in medical patients/public health
• ________ and conducting research
Anthony Biglan. (2015). The nurture effect: How the science of human behavior can improve our lives & our world. New Harbinger Publications, Inc.
Susan M. Schneider. (2012). The science of consequences: How they affect genes, change the brain, and impact our world. Prometheus Books.
Lauren Slater. (2004). Opening Skinner’s box: Great psychological experiments of the twentieth century. Norton.
Paul Kunkel. (2017). How to toilet train your cat: 21 days to a litter-free home (2nd ed.). Workman.
Ian Ayres. (2010). Carrots and sticks: Unlock the power of incentives to get things done. Random House.
Jeremy Dean. (2013). Making habits, breaking habits: Why we do things, why we don’t, and how to make any change stick. Da Capo Press.
Charles Duhigg. (2012). The power of habit: Why we do what we do in life and business. Random House.
Daniel Akst. (2011). Temptation: Finding self-control in an age of excess. Penguin Books.
Hilke Kuhlman. (2005). Living Walden Two: B. F. Skinner’s behaviorist utopia and experimental communities. University of Illinois Press.
Kelly McGonigal. (2012). The willpower instinct: How self-control works, why it matters, and what you can do to get more of it. Avery.
Roy Baumeister & John Tierney. (2011). Willpower: Rediscovering the greatest human strength. Penguin Press.
Chris Hardwick. (2011). The nerdist way: How to reach the next level (In real life). Berkley Books.
David L. Watson & Roland G. Tharp. (2014). Self-directed behavior: Self-modification for personal adjustment (10th ed.). Wadsworth
Edward P. Sarafino (2010). Self-management: Using behavioral and cognitive principles to manage your life. Wiley.
Burns, D. D. (2022). Feeling great: The revolutionary new treatment for depression and anxiety. PESI Publishing, Inc.