1. How are fear and anxiety defined, and how do they relate to respondent and operant conditioning?
2. What are two basic principles used to reduce fear and anxiety? Describe Jones’ (1924) work on removing conditioned fears.
3. Explain how to apply the relaxation techniques of progressive muscle relaxation, diaphragmatic breathing, attention-focusing exercises (3 types), and behavioural relaxation training.
4. Explain how to apply the exposure-based therapies of systematic desensitization and in vivo desensitization. Which procedure is more effective?
5. How are flooding, modeling (3 types), and virtual reality exposure applied?
How can a specific ______ be reduced using behaviour modification?
(Nesbitt, 1973)
- 24-year-old female student who had intense fear of __________ (escalaphobia)
- history:
• phobia developed 7 years previous: she had gone up an escalator with her family with no difficulty
• however, upon descending, she was afraid of the apparent ______
• her family forced her onto the escalator, and she experienced intense fear during the ride
- avoided all escalators and took the stairs or elevator instead
- she feared that the ________ would pull her down, so she would miss her step
- upon unexpectedly encountering an escalator during shopping once, she nearly vomited
- behavioural treatment program:
• met therapist at a large department store with four floors of escalators
• with “coaxing, reassurance, and a little physical _____” she stepped onto an escalator
- results:
• threatened to _____, was at the verge of tears, and clung tightly to the therapists’ shirt
• spent 27 minutes riding up and down escalators
• experienced a dramatic decrease in _______, and rode escalator alone
• at 6 month follow-up, she reported experiencing no anxiety (except on rare occasions when descending)
Fear: caused by a stimulus or situation that produces unpleasant physiological response (autonomic nervous system arousal, or _______) and cognitive appraisal
- about 10% of Canadians experience an anxiety disorder; about 25% will be diagnosed with anxiety in their lifetime
- comprised of both respondent conditioning and operant behaviours
- respondent conditioning: conditioned _________ response (CER)
e.g., sight of escalator (CS) → autonomic system arousal (CR)
- operant conditioning: escape or avoidance (________ reinforcement)
e.g., autonomic system arousal (SD) → avoiding escalator and taking stairs (behaviour) → relief (SR-)
- presenting a CS repeatedly without the US
- part of procedure to reduce CERs
- can help extinguish CRs associated with substance abuse
e.g., exposing person to situation or environment linked to drinking or having person hold an alcoholic beverage (CS) without drinking it (US)
- kinds of CSs:
• __ ____: real-life events, objects, or people
e.g., sitting on an airplane
• ________: mental representations of events, objects, or people
e.g., imagining sitting on an airplane
• ________: overt representation of events, objects, or people
e.g., looking at a picture of a person sitting on an airplane
- includes extinction: involves presenting the CS without the US
- trains the person to substitute a competing or incompatible behaviour for the CR when the CS is present
Mary Cover Jones (1924): How can conditioned fears be removed?
- was a student of J.B. Watson’s
- pioneered the use of behavioural techniques in therapy, and was called “the first behaviour _________” and “the mother of behaviour therapy”
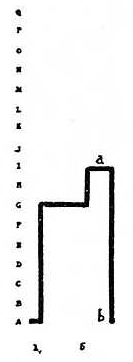
- Peter was a 3-year-old with average IQ (102)
- target behaviour: ____ reaction (screamed or cried, and fell flat on his back) in response to a white rat, a rabbit, a fur coat, a feather, and cotton balls
- listed 17 degrees of toleration:
A. Rabbit anywhere in the room in a cage causes fear reactions.
B. Rabbit 12 feet away in cage tolerated.
...
P. Fondles rabbit affectionately.
Q. Lets rabbit nibble his fingers.
- initial behavioural treatment program: “unconditioning” (respondent extinction)
• Peter observed behaviour of other children who did not have a fear of rabbits
• the other children played with the rabbit
- results:
• ________ to rabbit and modeling behaviour of others improved Peter’s tolerance (point a on graph)
• Peter then had scarlet fever and was in hospital for 2 months
• also, a big ___ jumped at him as he was returning from the hospital
• fear had regressed; _________ dropped (point b on graph)
- subsequent behavioural treatment program: “______ conditioning” (counterconditioning or stimulus substitution)
• a research assistant who Peter liked gave him a pleasant stimulus (food) which was associated with the rabbit
• eating and remaining calm were the competing responses
• Peter’s tolerance progressively increased over several weeks
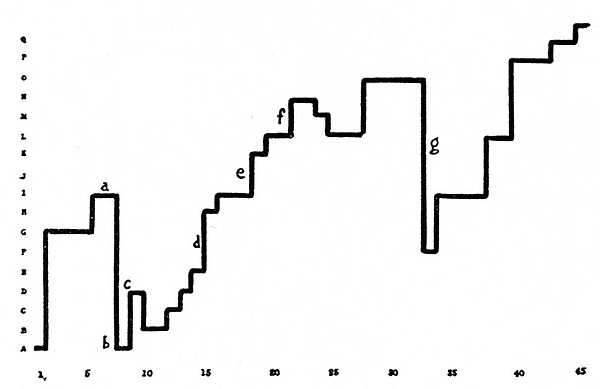
• brief drop in tolerance (point g on graph) caused by a slight _______ from the rabbit
• in the final session, Peter showed no fear--even when another child was disturbed by the rabbit
- Jones called this study a “______” to Watson’s experiment on Little Albert
- gained widespread acceptance in the 1970s
- __________: a state of calmness with low psychological and physiological arousal and tension
- setting should be comfortable, free of ____________ and interruptions
- person sits in a recliner or lies down in a comfortable position
- duration:
• sessions should last 10-30 minutes
• initial sessions will typically take longer as the person is ________ the technique
• time should be set aside for regular sessions every day
- person should be relaxed but alert at the end of the session; the goal is not for the person to fall ______
- person should record data on the intensity of the relaxation in each session on a data sheet
• ___________ ______ relaxation (PMR) (Jacobson, 1938; Bernstein & Borkovec, 1973)
- alternately tensing and relaxing different muscle groups while resting
- this leaves the muscles more relaxed than they were before
- can be used with children as young as 3 years of age to relieve fear and anxiety during dental treatment, for example
- follow-up assessments show that positive psychological and physiological results continue after treatment, and may even get ________ over time
• _____________ breathing (a.k.a. deep breathing)
- using the muscles of the diaphragm to breathe deeply and slowly in a rhythmic pattern, characterized by expansion of the abdomen instead of just the chest
- activates the parasympathetic nervous system
- during breathing, the person focuses on the act of breathing and its __________
- this behaviour is incompatible with the rapid, shallow breathing associated with high arousal and anxiety
- can be used in conjunction with other relaxation procedures
• _____ breathing (or “4-7-8 breathing”)
1. inhale through your nose for the count of 4
2. hold your breath for the count of 7
3. slowly exhale through your mouth for a count of 8
- this stimulates the _____ nerve, which activates the parasympathetic nervous system, directly slowing heart rate
- coherent breathing is effective for relieving stress and anxiety, and improving blood pressure (Priasmoro et al., 2025)
• _________-focusing exercises
▸ guided _______
- person imagines pleasant and peaceful scenes and images
- therapist guides the person through a script that describes what is experienced by each of the ______ in the situation
e.g., walking along a beach, or floating on a cloud
- attention is focused on the scene instead of anxiety-provoking thoughts and feelings
- can be done in person with a therapist or while listening to an audio recording
▸ _________ training (autogenic = “self-produced”) (Schultz, 1957)
- person imagines being in a pleasant and peaceful scene and experiencing specific bodily sensations, such as their arms feeling warm or heavy
- instructions specify which part of the body to focus on, what feeling to imagine; this is followed by a ____ period, and is repeated three times
- a full session involving all parts of the body takes about 35 minutes
- more suitable than progressive muscle relaxation for those people who have chronic pain or difficulty moving
- meta-analysis found improvements vs. controls; it also improved quality of life (Stetter & Kupper, 2002)
▸ __________
- the process of contemplating or focusing one’s attention on an object, event, or idea to help the person become detached or dissociated from their physical states, thoughts, and feelings
- derives from Eastern philosophy and religion; produces relaxation and mindful awareness of current __________
- essential components (Linton & Matteson, 2020):
1. quiet, distraction-free location
2. specific, comfortable posture
3. open ________
4. focus of attention
- focus can be on a meditation stimulus, like a visual object (e.g., a flower), a mantra (word-like sound), or person’s own breathing
- successfully applied to chronic pain by focusing on and separating physical sensations from the cognitive and emotional reactions to pain
- alleviates anxiety and depression to a similar degree as antidepressant drug therapy
- but low/no evidence of any effect on positive mood, substance use, eating habits, sleep, and weight (Goyal et al., 2014)
• behavioural __________ training (Poppen, 1998)
- involves relaxing different muscle groups, and adopting certain relaxed body postures
- similar to PMR, but does not include the muscle tensing component
- typically incorporates other relaxation procedures such as breathing exercises and focused attention
• systematic _______________
- developed by Joseph Wolpe (1958) based on Mary Cover Jones’ counterconditioning
- applied to reverse a person’s learned fear response (phobia or CER)
1. person first learns __________ techniques and exercises
2. person then develops stimulus _________ (or fear hierarchy) of CSs
▸ Subjective Units of __________ Scale (SUDS): 0-100 scale that is used to rate the amount of fear produced by a given CS (Wolpe, 1990)
▸ CSs are arranged in a hierarchy, from least fear-inducing to most fear-inducing
3. therapist describes a CS while the person maintains a state of __________
▸ starts with the least fear-inducing CS
▸ reciprocal inhibition: relaxation response decreases the fear response
▸ if the person can remain calm and relaxed, therapist moves on to the next most fear-inducing CS in the hierarchy
- evaluation:
▸ highly _________ in helping overcome fears
▸ effectiveness is maintained over time: follow-ups 2 years later reveal few recurrences in fears
▸ often improves other areas of emotional functioning
▸ also effective for other anxiety-related problems (e.g., paruresis or “shy bladder”) and compulsive behaviours (e.g., repeatedly checking to ensure doors are locked)
- controversies:
▸ not all research finds that relaxation enhances desensitization
▸ some studies using only the _________ CSs had as much success as those using the full hierarchy
• __ ____ desensitization (or gradual in vivo exposure, or graduated exposure)
- person is gradually exposed to the actual stimulus that is producing fear/anxiety
- similar to systematic desensitization; typically includes relaxation
- may be supplemented with _________ procedures, in which the person practices self-statements to cope with the situation and avoids statements that will make the anxiety worse
- evaluation:
▸ research shows it is effective for anxiety disorders (e.g., panic attack, specific phobias, social anxiety),
▸ obsessions (repetitive thoughts), and compulsions (repetitive, ritualistic behaviours)
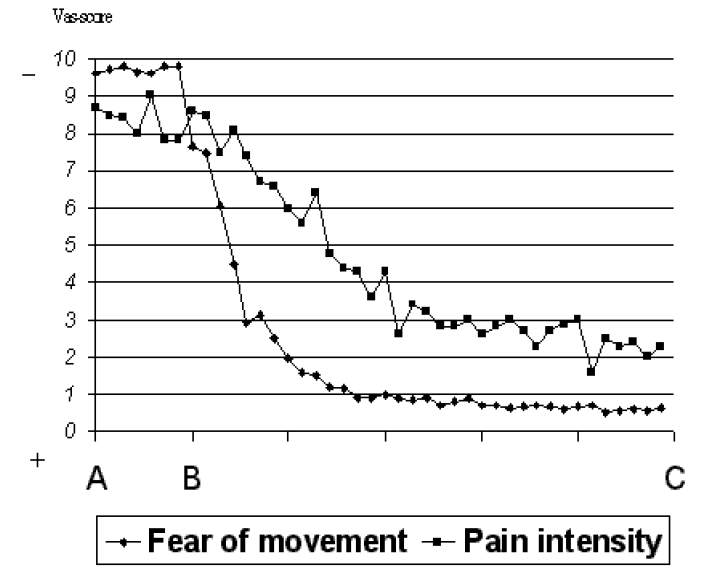
Vlaeyen et al. (2002):
- 45-year-old woman who had low back ____, due to degeneration of several lumbar discs in her spine
- medications, physical therapy, and chiropractic did not alleviate her pain
- target behaviour: fear of ________ and injury (kinesiophobia)
- fear of physical activity leads to avoidance of activities, which leads to further degradation of the condition
- behavioural treatment program: _________ exposure
▸ person was shown 98 photos of daily life (e.g., lifting, bending, walking, bicycling) from PHODA (Photograph series of Daily Activities)
▸ created hierarchy of items
▸ baseline phase: pain intensity was recorded, and pain-related fear was measured (using visual analog scale for pain)
▸ exposure treatment phase: therapist _______ an activity, then person performed the activity until her anxiety levels decreased
▸ she progressed through the hierarchy; pain and fear continued to be recorded
- results: substantial decreases in pain-related fear and, more slowly, ____ report
Comparing systematic & in vivo desensitization:
(David Barlow et al., 1969)
- female college students with fear of snakes (ophidiophobia)
- baseline: tested for fear with a “harmless boa constrictor” kept in a glass cage covered with a wire grating
- fear response measured two ways:
• ___________ measure: 17 behaviours, ranging from watching the snake in the cage from 15 feet away to picking up the snake
• _____________ measure: galvanic skin response (GSR) measured while the snake was at several different distances
- behavioural treatment programs:
• gp1: desensitization with imagined CSs
• gp2: desensitization with in vivo CSs
- results:
• in vivo (gp2) was able to complete more steps in the behavioural measure:
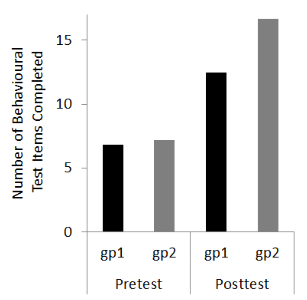
• in vivo (gp2) had lower GSR to items in the hierarchy:
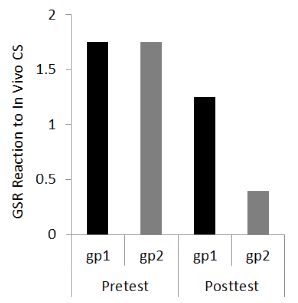
- conclusion: in vivo procedures are more _________ than imaginal procedures
• flooding
- client is exposed to a highly feared object or situation for a _________ period of time
- therapist ________ client from escaping or avoiding the situation
- anxiety is not reinforced; response is extinguished
- relaxation is not included
- can often be completed in a single session for specific fears
- some clients are not able to tolerate extremely intense exposures, so flooding should be carried out only by a ____________ behaviour analyst
- _________ therapy: uses imagined stimuli or situations (Stampfl & Levis, 1967)
• ________
- phobic person watches someone else performing a feared behaviour
- can desensitize fears vicariously
- different types:
▸ ___________ modeling
- person first observes someone else cope with increasingly feared situations
- the person is encouraged to join in
- is guided to increase contact with the feared object or event using verbal and physical guidance prompts
▸ _____ modeling
- person watches a video of someone else dealing with feared situations
- found to be effective in reducing patients’ anxieties about medical treatments such as surgery or invasive dental work
- however, watching a filmed model has been found to be less effective than participant modeling
e.g., Melamed and Siegel (1975):
- 4- to 12-year-old patients scheduled for surgery
- control film group watched Living Things are Everywhere which shows a boy going on a nature trip in the country
- hospital film group watched Ethan Has an Operation which shows the events encountered by a 7-year-old boy in the ________
- recorded GSR, self-reports of fear, and parents’ ratings of _________ behaviour
- measured the night before surgery and at 3-week follow-up
- hospital film group had lower GSR, lower fear, and fewer problem behaviours
▸ ________-_____ vicarious exposure
- person uses a computer to guide scenarios/CSs that an on-screen persona experiences
- not as effective as in vivo desensitization, but both methods produce durable reductions in fears
In general, teaching how to behave in fearful situations, and __________ that behaviour seem to be critical in overcoming fears.
A significant problem is that dropout rates in exposure therapy are as high as 45% (Choy et al., 2007). How can this be overcome?
• _______ _______ exposure therapy (VRET)
- participants wear a head-mounted stereoscopic virtual reality (VR) display that presents a three-dimensional, immersive experience that may include directional audio, haptic feedback/vibration, and scents
e.g., Virtual Iraq/Afghanistan uses modified version of the Xbox game Full Spectrum Warrior to treat veterans with post-traumatic stress disorder (PTSD) (McLay et al., 2012)
- presents a controlled, _________ experience as part of exposure therapy
- evaluation:
▸ highly effective in treating fear of heights (acrophobia)
has also been applied to fears and specific phobias including flying, storms, bridges, public speaking, needles, claustrophobia, driving, insects, and snakes
systematic reviews and meta-analyses reveal that VR is as effective as traditional exposure-based therapy in treating PTSD (Carl et al., 2019; Deng et al., 2019; Gonçalves et al., 2012)
may be more useful in treating clients who are _________ to traditional therapies