| International Journal of Qualitative Methods 4 (2) June 2005 |
Recruiting Transcultural Qualitative Research Participants: A Conceptual Model
Phyllis Eide and Carol B Allen
Phyllis Eide, PhD, RN, APRN, BC, Assistant Professor, Washington State University College of Nursing, Spokane, Washington
Carol B. Allen PhD, RN, Clinical Associate Professor, Washington State University, College of Nursing, Spokane, Washington
Abstract: Working with diverse populations poses many challenges to the qualitative researcher who is a member of the dominant culture. Traditional methods of recruitment and selection (such as flyers and advertisements) are often unproductive, leading to missed contributions from potential participants who were not recruited and researcher frustration. In this article, the authors explore recruitment issues related to the concept of personal knowing based on experiences with Aboriginal Hawai’ian and Micronesian populations, wherein knowing and being known are crucial to successful recruitment of participants. They present a conceptual model that incorporates key concepts of knowing the other, cultural context, and trust to guide other qualitative transcultural researchers. They also describe challenges, implications, and concrete suggestions for recruitment of participants.
Keywords: research recruitment, transcultural, qualitative research, knowing, trust, culture
Citation Information
Eide, P., & Allen, C. B. (2005). Recruiting transcultural qualitative research participants: A conceptual model. International Journal of Qualitative Methods
Authors' Note
Many thanks to Drs. Ruth Bindler and Dawn Doutrich, Washington State University College of Nursing, for reviewing this article.
Transcultural qualitative researchers encounter many challenges in planning and implementing their research. If research is to benefit the participant group, it must be designed and implemented in conjunction with community or group members and leaders (Kowalsky, Verhoef, Thurston, & Rutherford, 1996). Collaborating with community members is an essential first step that is eased when the researcher knows and is known by community members and leaders. In cultures such as those of Aboriginal Hawai’ians and Micronesians, knowing and being known are crucial to every activity. (Aboriginal as used here refers to the original inhabitants of a place.) Daily comments such as “I know her,” “I know her auntie,” “He knows my uncle,” and “He knows the governor” reveal the truth of the adage “It’s not what you know but who you know” in these and many other cultures.
Our purpose in this article is to describe our experiences and challenges in recruiting participants and conducting transcultural research in Hawai’i and Micronesia and to share a model for planning and implementing qualitative research that might provide guidance to other transcultural researchers. Central to this model is the concept of knowing the person as described by Tanner, Benner, Chesla, and Gordon (1993).
When Phyllis joined the faculty of the Washington State University College of Nursing in fall 2002 after nearly 20 years in Hawai’i, she was delighted to find a colleague who had also spent time in the Pacific. Carol taught at the University of Guam from 1992 to 1996 and was in the process of completing her doctoral dissertation on nursing leadership in Micronesia. Phyllis had completed her doctoral dissertation research in 2000 on Native Hawai’ian women and breast cancer. During the course of many conversations on our mutual experiences in doing research in the Pacific cultural milieu, we became intrigued with the challenges and guiding values that undergirded both of our experiences in recruiting participants from diverse cultures. The complexity of establishing researcher-to-participant relationships across cultures, which at the heart is a human-to-human connection, motivated us to share our experiences in this article. The concepts of context, knowing and being known, and trust emerged as constructs for a model that we present in this article. Because the model emerged from our shared experiences, we begin with a recounting of these experiences in recruiting qualitative research participants in Hawai’i and Micronesia.
I conducted my research with Aboriginal Hawai’ian women and breast cancer in the late 1990s in the state of Hawai’i. I was confident that my many years of experience living and working in Hawai’i, plus my professional and personal contacts with the Native Hawai’ian community, would ease the issue of recruitment for this research. At that time, my immediate supervisor at the local university’s baccalaureate nursing program was part Hawai’ian, and her husband was the director of the local federally funded Native Hawai’ian health clinic. I planned to identify potential participants from the clinic’s registry and send out an invitation letter with both my signature and that of the clinic director. In addition, I recruited a coresearcher from the Native Hawai’ian culture who shared ideas on how to reach the women and who had her own connections to the community.
However, as with many qualitative transcultural projects, these initial assumptions proved to be faulty. When registering new patients, the Native Hawai’ian health clinic recorded as a diagnosis the word “cancer” rather than specifying the type of cancer. This proved to be an insurmountable barrier to the original plan of sending out invitation letters directed at breast cancer survivors. Printed materials with the project logo, which were developed with the help of the coresearcher, were handed out at appropriate health fairs and community gatherings. However, these efforts did not yield any recruits to the study.
Although these challenges appeared to produce a rather dismal forecast for recruitment, there were more subtle forces at work that led to a change of direction and a new commitment to flexibility in recruitment design. Through my work supervisor’s personal contacts, three potential participants were identified, contacted, and recruited. In addition, the registered nurse who worked at the clinic and who had known this patient population for a number of years became aware of my study and offered to facilitate contact with a number of women that fit the profile for the study, and who might be interested in participating. In this manner, 7 more women were recruited and interviewed. Finally, a contact was made on Oahu via one of the original Hawai’i Island participants, who indicated that her cousin also fit the profile and might be willing to join the study.
In this instance, original plans to recruit study participants through traditional means of letters and posters/flyers proved to be unsatisfactory. The critical turning point was my supervisor’s connecting me to the clinic nurse, who knew the client population and was known and trusted by them. Without her brokering between the cultures of university and researcher (me) and Native Hawai’ians and breast cancer population (clinic), the study would have not been accomplished within the 1-year time frame that it encompassed. The one instance of classic snowballing was the referral to the Oahu-based cousin. In addition, within the study, participants were asking me, “Have you talked to ‘X’”? This comment reflected a precursor stage to snowballing. However, in all cases, the recommended participant was already in the study. This illuminated the close connections and contacts people have with each other on the island of Hawai’i (which, although the largest island in Hawai’i State, has a very rural population).
My research was conducted in 2001 primarily with individual nursing leaders I had come to know well through collaboration on a number of educational and service projects conducted over a 4-year period (1992-1996) as a faculty member at the University of Guam. I also participated in four annual meetings of the American Pacific Nurse Leaders Council (APNLC), to which all the participants belonged. My initial introduction to these nurses was facilitated by three well-respected nursing leaders: the White American Dean of the College of Nursing and Allied Health, a Micronesian nurse leader who was one of the founding members of APNLC, and a White nursing faculty member who had lived and worked in Micronesia for more than 20 years.
Through repeated contacts and sustained interactions, the Micronesian nurses and I came to know one another. We shared both professional activities and recreation together. I met many of their families, and we shared our lives and our interests. Throughout my interactions with them, I endeavored to demonstrate respect, humility, and willingness to learn and to consider new ideas, perspectives, foods, and activities. In the beginning, I listened much more than I spoke, seeking to understand their culture, lives, and worldviews. I carefully considered their ideas and endeavored to avoid imposing my own. I presented myself as a student of their ways as I worked to become as culturally competent as possible.
After I left the University of Guam and returned to the mainland United States in 1996, I continued to correspond with some of the nurse leaders and to attend the leadership meetings whenever possible. When I told the nurses I wanted to hear their leadership stories because I believed that other nurses could learn from them, they were concerned that they had little to teach. Nevertheless, they were excited about an opportunity to share their stories so that others would learn about their islands and their experiences as leaders. They were delighted when I told them I would return to share the interpretations and seek their help in validating my findings.
With the exception of three of the retired nurses, I had previously worked with and knew each of the participants in my study. Most participants were contacted and interviewed during the APNLC meeting in 2001 in Chuuk state, Federated States of Micronesia (FSM). I contacted the remainder by phone or e-mail on their home islands and made arrangements to meet with them in a place of their choosing. Of the three people included in the study that I had not previously met, all but one knew about me from mutual acquaintances. The one person who was not acquainted with me asked who else I was interviewing for the study. When I mentioned the names of two widely respected nurses from her community, she immediately said, “Oh, well in that case I will be happy to talk to you.” In the end, I was given more names and volunteers for the study than I could manage.
I attribute the success in recruiting these participants to relationships that we built over time and to the trust and generosity of these women. The level of disclosure in the interviews indicated that the nurses trusted me enough to share experiences that reflected both positively and negatively on themselves, their health care systems, their governments, and their cultures. Arranging to do the interviews at the annual meeting where family and work obligations were significantly less than on the women’s home islands might also have contributed to their willingness to participate. In 2003, I returned to share and validate my interpretations of the interviews with the women and was warmly received.
In our discussions of these experiences of planning research and recruiting participants, three common concepts emerged: context, trust, and knowing the person. Articulation of these concepts led to the development of a model that we believe might provide guidance to other researchers engaged in qualitative transcultural research. This model will be presented later in the article.
People make sense of the world and decide on appropriate responses to the environment through their particular cultural lenses. An individual’s culture is largely invisible or unconscious to that person (Giger & Davidhazar, 2004). Interactions in all cultures are governed by unstated rules arising from the culture’s history, values, and social structure. These rules are taken for granted by culture members but are often unfathomable to outsiders. Hall (1976) classified cultures as high or low context based on the relative importance of the social situation in determining and interpreting behaviors.
In low-context cultures, communication is explicit. In most situations, individuals are expected to communicate information, needs, and expectations directly. The dominant culture of the United States, by virtue of its diversity and heterogeneity, is relatively low context. The dominant U.S. culture is also individualistic. The needs of the individual are paramount, and individual action and accountability are the desired norm (Hall, 1976; Kim, 1994).
In contrast, Pacific Island cultures tend to be high context and collectivistic. Because these cultures are more homogenous, interactions are governed by rules and expectations that are embedded in the social context (Hall, 1976). These implicit rules and expectations are often baffling to the outsider, who does not share the “insider’s” frame of reference. Communication is implicit, and meanings are interpreted primarily from the context and from nonverbal cues (Kim, 1994). High-context cultures tend to be collectivist, focusing on the needs and concerns of the group: the family, clan, or social or work unit rather than the individual.
When researchers and participants have widely disparate cultural norms, the researchers’ humility, cultural sensitivity, and caring contribute to building a bridge of trust among them. The researcher demonstrates cultural sensitivity and competence through knowing key values and stakeholders, and exhibiting culturally appropriate communication and willingness to learn (Laverack & Brown, 2003). Researcher-participant relationships are sustained through continued personal connection, respect, reciprocity, feedback, and long-term maintenance (Brach & Fraser, 2000).
Trust is central to the success of any relationship, including those between participants and researchers (Hardin & McFarland, 2000; Pletsch, Howe, & Tenney, 1995; Shavers, Lynch, & Burmeister, 2002). Trust includes faith that the other person will follow through on obligations, behave reliably, and exhibit integrity. Preconditions to trust include communication, reliability, consistency, respect, competence, trustworthiness, knowing one another, and negotiation (Lynn-McHale & Deatrick 2000).
Trust can be gained or lost but is never static. Developing trust usually requires repeated interactions over time, in the context of a long-term relationship (Corbie-Smith, Thomas, & St. George, 2002; Lynn-McHale & Deatrick, 2000). Trust building demands time and sensitivity to issues that might be raised, as well as being prepared for the unexpected (Kowalsky et al., 1996). “Being there and being seen” by immersing oneself in the community and contributing to the community is one means of developing trust and credibility (Meadows, Langendyk, Thurston, & Eisener, 2003; Sixsmith, Boneham, & Goldring, 2003). In addition to having cultural knowledge and cultural sensitivity, collaboration with the community toward mutually desirable goals is an essential component in the conduct of culturally competent research (Sawyer et al., 1995). Developing mutual goals and plans requires that the researcher and the community of potential participants know one another.
Developing trust is both more difficult and more crucial when researcher and participant do not share the same culture. When the researcher is a member of a group that has historically been an oppressor or colonizer of the potential participant group, then trust building is more complicated and difficult, and requires more time (Corbie-Smith et al., 2002; Lindenberg, Solorzano, Vilaro, & Westerbrook, 2001). Both Micronesia and Hawai’i were colonized by the United States. One of the consequences was that the colonizers, although fewer in number, were more powerful than the original inhabitants because they were for many years perceived to possess more advanced knowledge, skills, and desirable resources or goods. Many Micronesians learned from their parents and teachers that Americans (and other Westerners) “know more than we do” (Allen, 2003; Souder, 1992). Health care systems in Micronesia and Hawai’i were designed and are largely financed by private industry and/or the U.S. government. This contributes to the persistence of power inequalities and distrust between the Aboriginal inhabitants and dominant culture Americans.
Research processes and outcomes are not always viewed positively by Aboriginal communities. Many groups such as Native Hawai’ians and Micronesians experienced exploitation when White Ha’ole researchers came to their communities to collect data to achieve the researchers’ personal and professional goals without sharing the results and benefits of the research with the group that was studied. Thus, research participants were unable to identify how the research benefited or disadvantaged them. These experiences resulted in a great deal of resistance to participation in research among members of these groups. Consequently, the researchers must demonstrate that they can be trusted to listen to suggestions and information from community members and potential participants. They must also develop concrete plans for making the results available to the participants’ communities in a way that the community finds accessible and allows the participants to validate the findings.
Invoking an appropriate bioethical stance toward Aboriginal peoples calls for respect for the individual and culture (Ellerby, McKenzie, McKay, Gariépy, & Kaufert, 2000). Respectful communication is crucial to trust development (King, 2002). In addition, it must be culturally appropriate. This type of communication incorporates verbal and nonverbal styles that participants perceive as suitable to each party’s roles and the context of the interaction. Not only must the researcher know about the group being studied, he or she must also be known by at least some group members to gain access that allows for trust building (Morse & Field, 1995). Numerous and varied connections with community members of the culture are helpful. Prospective participants will often seek to identify people who are known by both the participant and the researcher as a means of checking credibility and trustworthiness. Trust is strengthened when issues of concern to the participants are addressed and they are engaged as valued, informed, and active members of the study (Picot et al., 2002).
Nurses acknowledge the importance of knowing the person in providing care to their patients (Jenny & Logan, 1992). Expert nurses consistently described knowing the patient as crucial to the exercise of skilled clinical judgment (Tanner et al., 1993). Nurses who knew the patient treated each person as a unique individual embedded in a distinct context. These nurses grasped the meaning of situations for individual patients and identified subtle cues that helped them recognize and respond to specific patient needs (Radwin, 1996; Tanner et al., 1993). Conversely, the negative effects of not knowing the patient might include depersonalization, increased vulnerability, and decreased trust (Whittmore, 2000).
The concept of knowing the patient as presented by these authors was unidirectional, in that the nurse was described as knowing the patient, but there was no consideration of the reciprocal need for the patient to know the nurse. Nevertheless, it is evident that if the patient is to trust the nurse, he or she must come to know the nurse as a person, at least in a professional context. Although the nurse might share less personal information than the patient does, some sharing of personal context occurs, and patients observe the nurse and decide whether he or she is competent and trustworthy. Similarly, participants and qualitative researchers must come to know one another to develop a trusting relationship that fosters sharing of sensitive information.
These relationships with individuals and communities in qualitative research are characterized by mutual sharing or reciprocity (Dobson, 1989). The format and content of the sharing essential to building relationships varies among and within cultural groups. Different groups define personal information in multiple ways that are grounded in the values of those particular cultures. What is considered private in one culture might not be so in another. For example, in the dominant U.S. culture, many people consider finances private, whereas in some Asian cultures, people might share financial information readily but be reluctant to talk about family matters with people they do not know well. Dominant U.S. culture tends to be task focused and oriented to clock time and schedules. An appointment to meet someone usually means the parties have a certain task or activity to perform. We like to “get down to business” and finish on time. In contrast, in many cultures, including Polynesian and Micronesian, the relationship is far more important than the task (Palafox & Warren, 1980). People get together simply to be together and share time with one another. Clock time might be irrelevant; meetings take as long as is needed by both parties and usually begin with sharing about family and community rather than business. Researchers must come “to know” the culture and the individual participants. This is a process that takes time, flexibility, and willingness to learn.
Knowing the community occurs in both formal and informal ways. One of the major ways to develop such knowledge is the formation of community partnerships (Lindenberg et al., 2001). Relationships with stakeholders foster community partnerships. Stakeholders can be defined as “anyone with an interest” in the particular community and might include residents, service providers, business people, and formal and informal group leaders (Sixsmith et al., 2003). Stakeholders provide important links with the community. They can assist astute researchers in identifying and responding to community issues. They also function as gatekeepers who control access to other community members (Groger, Mayberry, & Straker, 1999; Sixsmith et al., 2003).
Another term that can be applied to these individuals is that of culture broker (Jezewski, 1993). These brokers understand and are sympathetic to the values and issues of each of the relevant cultures. Culture brokers are people that serve as links between individuals or groups who are culturally different. Using skills such as advocacy, negotiation, and mediation, culture brokers bring people together and reduce misunderstandings and conflict (Jezewski, 1990). People acting as culture brokers can vouch for the researcher and facilitate contact with potential participants, or they can deny access.
One approach to recruitment is to ask the culture broker to refer clients to participate in a study. In the process of snowballing, the researcher or the culture broker starts with a known group of people and recruits more participants through contacts of those original group members. In this way, each contact leads to another, thereby enlarging the potential pool of participants (Miles & Huberman, 1994). This is an effective method of helping the researcher to be known to others by the process of positive recommendation. It can occur in a variety of social settings, such as clinics, churches, and social clubs (Okazaki & Sue, 1995). Snowballing provides opportunities for the culture broker and participants to vouch for the cultural competency of the researcher to new contacts. Other advantages of this method include the identification of other key contacts and helping to balance the power relations between researcher and participant (Crist & Escandón-Dominguez, 2003). One drawback to this method is the tendency to recruit people who resemble each other, limiting the diversity of the sample (Miles & Huberman, 1994; Sixsmith et al., 2003).
As we discussed the concepts of trust and of knowing and being known in the context of a multicultural environment, we began to see how they might relate in a visual fashion.
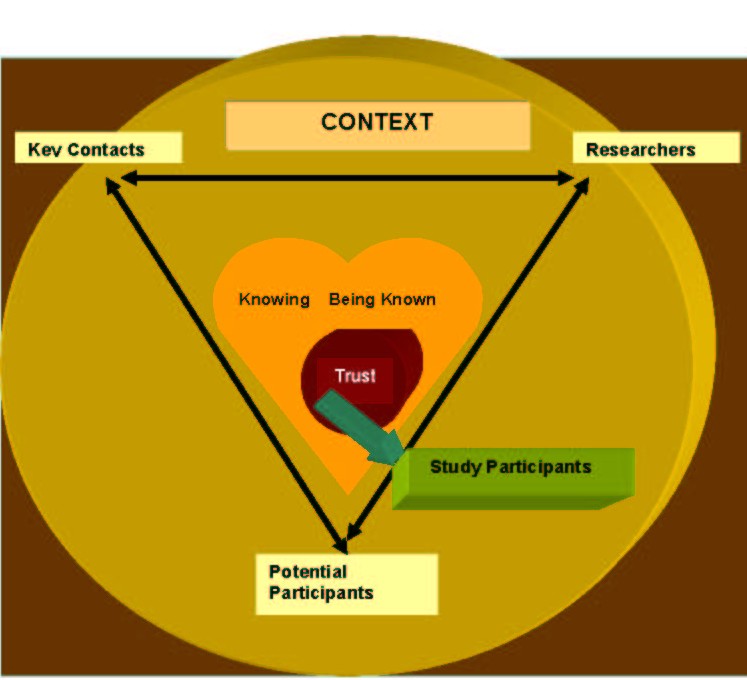
In the model (Figure 1), context is the milieu in which researchers, key contacts, and potential participants interact. Context encompasses the cultures, values, and needs of all the players. The interaction of the players is active, continuous, and reciprocal. Through their relationship, the individuals and groups come to know and be known by one another. This process leads to either trust or mistrust. When trust is developed, it becomes the bridge between researcher and participant.
Figure 1: A Conceptual Model for the Recruitment of Transcultural Research Participants
 We worked in the communities where our research was conducted and came to know and understand individual community members and their cultures. Simultaneously, community members came to know and understand us as individuals and as members of the academic and nursing community. In some cases, our community work put us into direct contact with potential participants. In other cases, our work in the community brought us into contact with key people who served as culture brokers by connecting us with potential participants, vouching for our credibility and trustworthiness, and helping us to become more culturally competent. In both Hawai’i and Micronesia, new people we met would often exclaim, “I know you!” meaning they knew us by reputation or they knew someone who knew us. When we met people who “knew” us in this way, trust was built more quickly than when we were totally unknown to the individual.
We worked in the communities where our research was conducted and came to know and understand individual community members and their cultures. Simultaneously, community members came to know and understand us as individuals and as members of the academic and nursing community. In some cases, our community work put us into direct contact with potential participants. In other cases, our work in the community brought us into contact with key people who served as culture brokers by connecting us with potential participants, vouching for our credibility and trustworthiness, and helping us to become more culturally competent. In both Hawai’i and Micronesia, new people we met would often exclaim, “I know you!” meaning they knew us by reputation or they knew someone who knew us. When we met people who “knew” us in this way, trust was built more quickly than when we were totally unknown to the individual.
As researchers, we consulted with the potential participants to identify with them the benefits of the studies for the group. More important, however, we needed to understand and adapt our approach to the cultural context of the potential participants. This was a delicate process that took time, effort, and flexibility. For example, Phyllis worked closely with her Hawai’ian coresearcher to develop a logo based on a cultural proverb. This logo was used on all study materials and on the gift provided to each participant.
We established foundations for trust with potential participants both through face-to-face interactions with them and indirectly, with the help of local leaders and culture brokers. In addition to considerations related to the participants’ cultural context, we had to take into account factors within the culture of research. Researchers working in the United States or with U.S.-based organizations are required to obtain approval for research from their organization’s institutional review board (IRB) and to adhere to regulations arising from the Health Insurance Portability and Accountability Act (HIPAA) (U.S. Department of Health and Human Services, Office for Civil Rights, 2003). This act affects researchers’ access to health information and to potential participants (Olsen, 2003). If HIPAA had been in effect at the time of Phyllis’s study, the clinic nurse would have been required to ask patients to contact the researcher directly or to sign a consent allowing the nurse to share Individually Identifiable Health Information (IIHI) with Phyllis to identify them as cancer patients. The provisions of this act provide important safeguards for patient privacy but might also create obstacles in transcultural research. Many cultures have little or no concept of confidentiality. People live together in community and expect that everyone knows what is happening with members of that community without asking. In some cultures, for example Yap State in Micronesia, community members are expected to “know” the problems their neighbors are experiencing (A. Boliy, personal communication, June 18, 2003). In cultures in which the traditional preferred mode of communication is oral, written confidentiality agreements might carry little weight. Assurances by trusted community members acting as culture brokers might be even more important than they were prior to the implementation of these requirements. In addition, since the implementation of HIPAA, the complexity of consents has increased and their readability decreased (Hochhauser, 2002). Although consents and privacy statements can be written in simple terms, different IRBs respond differently to the same consent (Larsen, Bratts, Zwanziger, & Stone, 2004). It is likely that some IRBs are more comfortable with complex and legalistic statements that clearly mirror the provisions of HIPAA.
We will now summarize by sharing the challenges we found and lessons we learned through this process in the framework of the three common concepts of context, trust, and knowing.
It is crucial for those engaged in transcultural research to develop a deep and significant appreciation of the culture and its influence on potential research participants. Ideally, the researcher’s academic study of the culture will be matched with firsthand observation and immersion in the cultural milieu for extended periods. Many subtle cultural nuances can be absorbed only by first-person experiential learning, not by reading books or articles.
Researchers and participants engaged in transcultural inquiry enter into a relationship that is reciprocal and mutual. Sharing the research findings with participants and the community helps complete the research process in a way that can continue to build trust and knowledge. This is especially important for cultures that have been part of research projects whose findings were not shared with participants or (worse yet) were misinterpreted by researchers.
A natural outgrowth of this process is for the transcultural researchers to give back to the community and culture in a meaningful way. Spending time working on community projects originated and managed by community members is one way to contribute on their terms, to develop trusting relationships, and to determine what matters to the community.
For the qualitative transcultural researcher, it will always be a challenge to be present in the community for a sufficient length of time for mutual trust to develop through knowing and being known. If that time is foreshortened, it becomes imperative that the researcher establish connections with key people within the culture who can vouch for the project’s (and researcher’s) credentials and worth. In addition, the researcher must demonstrate that she or he is trustworthy.
One key element to this process is to gain the support of key members of the culture who are mutually trusted by researcher and potential participants. Identifying and connecting with these key stakeholders should ideally begin early in the process. Other challenges include identifying and resolving misunderstandings that can arise from a lack of common cultural referents, and those issues that spring from the power imbalance between researcher and participant.
In addition to the ways of knowing and being known discussed above, our advice to those researchers who wish to engage in this type of study is first to know your own culture and be secure enough in that knowledge that you do not wish to claim another’s culture for your own. The skills of listening and observing in a spirit of humility are crucial to this type of research process. They will help uncover the cultural and community issues that are congruent with the aims of the study; such connections will help researcher and participants develop a clear link between their experiences and the research.
Finally, researchers must be willing to be flexible in terms of recruitment method. Key informants are pivotal elements in recruitment and might be found outside traditional Westernized power structures. Their power base might be clan or kin relationship, or based on some subtle nuance of cultural context that might not be overtly apparent to the outsider.
Things can and will go wrong throughout the process of entering a community and planning and implementing the research. Researchers invariably make mistakes and sometimes alienate key people. A spirit of humility and willingness, accompanied by genuine care and concern for the well-being of the people in the community, can go a long way toward redeeming these errors. Nevertheless, despite the researchers’ best efforts and intent, sometimes trust is not built or is destroyed. When this happens, it is not possible to continue the research without at the very least a lengthy waiting period and continuous efforts to rebuild trust. If rebuilding trust is not possible, the researcher must reevaluate and perhaps select another population for study.
Conducting transcultural research contains many joys as well as challenges. Recruiting participants can be an experience that runs the gamut from disheartening and discouraging to that of excitement and fulfillment. Being aware of some of the key elements we found useful in our experiences will be helpful in guiding other qualitative researchers as they prepare to conduct research in a transcultural milieu.
Allen, C. (2003). The lived experience of Micronesian nurse leaders (Doctoral dissertation, Gonzaga University). Dissertation Abstracts International, 64/09, 4280.
Brach, C., & Fraser, I. (2000). Can cultural competency reduce racial and ethnic health disparities?: A review and conceptual model. Medical Care Research and Review, 57 (Suppl. 1), 181-217.
Corbie-Smith, G., Thomas, S., & St. George, D (2002). Distrust, race and research. Archives of Internal Medicine, 162(21), 2458-2463.
Crist, J. & Escandón-Dominguez, S. (2003). Identifying and recruiting Mexican-American partners and sustaining community partnerships. Journal of Transcultural Nursing, 14(3), 255-271.
Department of Health and Human Services, Office for Civil Rights. (2003). Standards for privacy of individually identifiable health information. U.S.C Fed. Reg., Title 45, § 160, 164. Retrieved October 29, 2004, from http://www.hhs.gov/ocr/hipaapre.html
Dobson, S. M. (1989). Conceptualizing for transcultural health visiting: The concept of transcultural reciprocity. Journal of Advanced Nursing, 14, 97-102.
Ellerby, J., McKenzie, J., Mc Kay, S., Gariépy, G., & Kaufert, J. (2000). Bioethics for clinicians, 18: Aboriginal cultures. Canadian Medical Association Journal, 163(7), 845-850.
Giger, J., & Davidhazar, R. (2004). Transcultural nursing: Assessment and intervention (4th ed.). St. Louis, MO: C. V. Mosby.
Groger, L., Mayberry, P., & Straker, J. (1999). What we didn’t learn because of who would not talk to us. Qualitative Health Research, 9(6), 829-835.
Hall, E. (1976). Beyond culture. New York: Anchor Books, Doubleday.
Hardin, J., & McFarland (2000). Avoiding gender and minority barriers to NIH funding. Journal of Nursing Scholarship, 32(1), 83-86.
Hochhauser, M. (2002). The effects of HIPAA on research consent forms. Patient Care Management, 17(5), 6-7.
Jenny, J., & Logan, J. (1992). Knowing the patient: One aspect of clinical knowledge. Image: Journal of Nursing Scholarship, 24(4), 254-258.
Jezewski, M. (1990). Culture brokering in migrant farmworker health care. Western Journal of Nursing Research, 12(4), 497-513.
Jezewski, M. (1993). Culture brokering as a model for advocacy. Nursing and Health Care, 14(2), 78-89.
Kim, U. (1994). Individualism and collectivism: Conceptual clarification and elaboration. In U. Kim, H. Triandis, K. Cigdem, C. Sang-Chin, & G. Yoon (Eds.), Individualism and collectivism (pp. 19-40). Thousand Oaks, CA: Sage.
King, T. (2002). Racial disparities in clinical trials. New England Journal of Medicine, 346(18), 1400-1402.
Kowalsky, L., Verhoef, M., Thurston, M., & Rutherford, G. (1996). Guidelines for entry into an Aboriginal community. Canadian Journal of Native Studies, 16, 267-282.
Larsen, E., Bratts, T., Zwangziger, J., & Stone, P. (2004). A survey of the IRB process in 68 U.S. hospitals. Journal of Nursing Scholarship, 36(3), 260-264.
Laverack, G., & Brown, K. (2003). Qualitative research in a cross-cultural context: Fijian experiences. Qualitative Health Research, 13(3), 333-342.
Lindenberg, C., Solorzano, R., Vilaro, F., & Westerbrook, L. (2001). Challenges and strategies for conducting intervention research with culturally diverse populations. Journal of Transcultural Nursing, 12(2), 132-139.
Lynn-McHale, D., & Deatrick, J. (2000). Trust between family and health care provider. Journal of Family Nursing, 6(3), 210-230.
Meadows, L., Langendyk, L., Thurston, W., & Eisener, A. (2003). Balancing culture, ethics and methods in qualitative health research with aboriginal peoples. International Journal of Qualitative Methods, 2(4), Article 1. Retrieved May 2, 2004, from http://www.ualberta.ca~iiqm/backissues/2_4/pdf/meadows/pdf
Miles, M. B., & Huberman, M. (1994). Qualitative data analysis. Thousand Oaks, CA: Sage.
Morse, J., & Field, P. (1995). Qualitative research methods for health professionals (2nd ed.). Thousand Oaks, CA: Sage.
Okazaki, S., & Sue, S. (1995). Methodological issues in assessment research with ethnic minorities. Psychological Assessment, 7(3), 367-375.
Olsen, D. (2003). HIPAA privacy regulations and nursing research. Nursing Research, 52(5), 344-348.
Palafox, N., & Warren, A. (Eds.). (1980). Cross-cultural caring: A handbook for health professionals in Hawai’i. Honolulu: University of Hawai’i Press.
Picot, S., Tierney, J., Mirpourian, N., Ericksson, J., Wright, J., & Powel, L. (2002). Engaging Black older adults and caregivers in urban communities in health research. Journal of Gerontological Nursing, 28(2), 19-27.
Pletsch, P., Howe, C., & Tenney, M. (1995). Recruitment of minority subjects for intervention research. Image: Journal of Nursing Scholarship, 27(3), 211-215.
Radwin, L. (1996). “Knowing the patient”: A review of research on an emerging concept. Journal of Advanced Nursing, 23, 1142-1146.
Sawyer, L., Regev, H., Proctor, S., Nelson, M., Messias, D., Barnes, D., et al. (1995). Matching versus cultural competence in research: Methodological considerations. Research in Nursing and Health, 18, 557-567.
Shavers, V., Lynch, C., & Burmeister, L. (2002). Racial differences in factors that influence the willingness to participate in medical research studies. Annals of Epidemiology, 12, 248-256.
Sixsmith, J., Boneham, M., & Goldring, J. (2003). Accessing the community: Gaining insider perspectives from the outside. Qualitative Health Research, 13(4), 578-589.
Souder, L. M. T. (1992). Daughters of the Island: Contemporary Chamorro women organizers on Guam. Lanham, MD: University Press of America.
Tanner, C., Benner, P., Chesla, C., & Gordon, D. (1993). The phenomenology of knowing the patient. Image: Journal of Nursing Scholarship, 25(4), 273-280.
Whittmore, R. (2000). Consequences of not “knowing the patient.” Clinical Nurse Specialist, 14(2), 75-81.
| International Journal of Qualitative Methods 4 (2) June 2005 |